
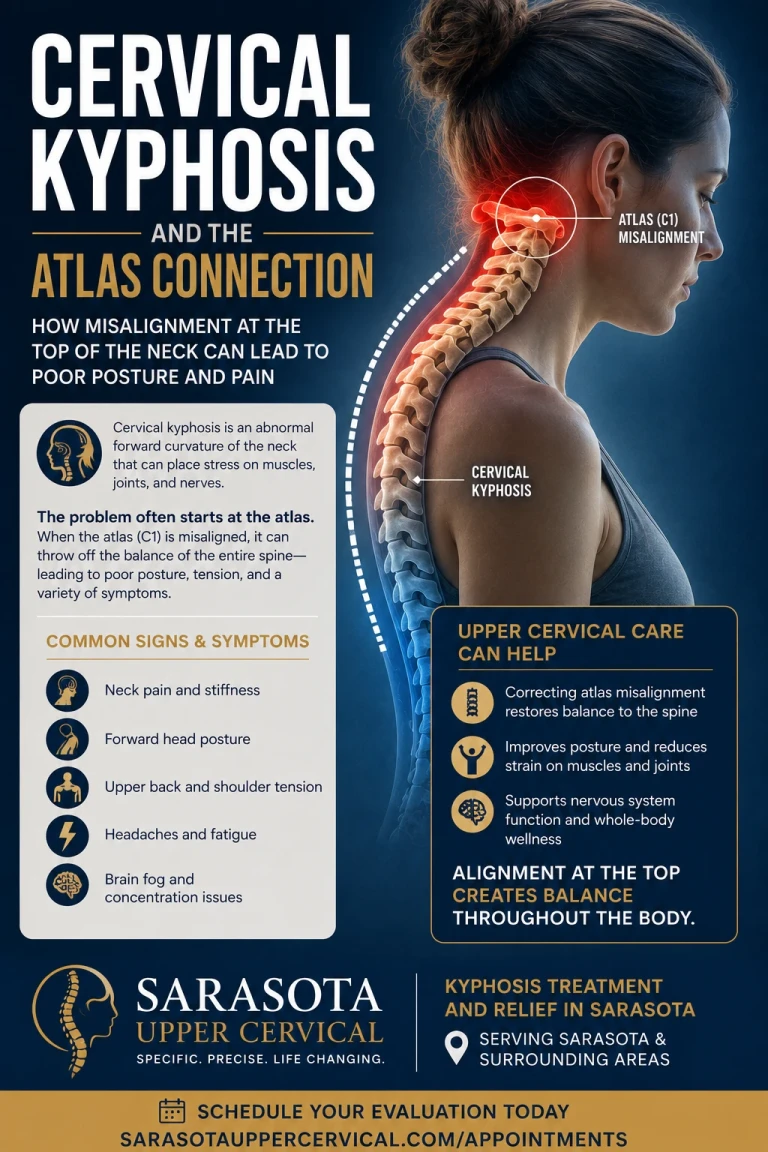
A healthy neck curves gently forward. When that curve flattens, straightens, or reverses into a backward bend, it's called cervical kyphosis, and it's one of the most common structural changes we see in people with chronic neck pain, headaches, mid-back pain, and even numbness and tingling down the arms. The standard explanation is "bad posture from phones and desks." That's part of it. But it leaves out the more important question: what controls the muscles that hold your head and neck in the first place? The answer points to the very top of the neck, the atlas, and explains why cervical kyphosis so often resists the usual stretches and ergonomic fixes.
This article covers what cervical kyphosis is, how the upper neck acts as the control center for postural muscle tone throughout the body, how an atlas misalignment can pull the head forward or flatten the curve, and the cascade of symptoms that follows, including arm numbness and tingling from scalene entrapment of the brachial plexus, and mid-thoracic pain from forward head carriage. Throughout, one boundary stays clear: some kyphosis is structural and requires medical care, and upper cervical chiropractic focuses on the postural and mechanical contributors rather than claiming to cure the condition.
Schedule Your Appointment
Schedule appointmentWhat cervical kyphosis actually is
The cervical spine is built with a forward curve (lordosis), a gentle C-shape that lets the head sit balanced over the shoulders and absorb load efficiently. Cervical kyphosis is the loss or reversal of that curve: the neck flattens (hypolordosis), straightens (a "military neck"), or bends the wrong way (a reversed or kyphotic curve). It exists on a spectrum, and small degrees are extremely common in the modern population.
The reason it matters is mechanical. When the head drifts forward of its balance point, the load on the neck rises sharply, and the body is forced into a chain of compensations. As forward head posture develops, the body responds with upper cervical extension, lower cervical flexion, and exaggerated thoracic kyphosis — all to keep the head in front of the center of gravity while still holding the eyes level and forward. That compensation chain is the engine behind the symptoms we'll discuss. But the compensation has to be triggered and held by something — and that's where the control system comes in.
The upper neck: the control center for postural muscle tone
Here is the piece most discussions of kyphosis leave out. Your postural muscles — the ones that hold your head, neck, and upper back in position — don't set their own tension. Their resting tone is governed by a sensory control system, and the headquarters of that system sits at the very top of the neck.
The suboccipital muscles just beneath the skull carry one of the highest densities of muscle spindles in the body — sensory organs that constantly report the position of the head. The upper cervical spine as a whole holds one of the highest concentrations of proprioceptive receptors anywhere in the body, making it a key contributor to postural control and motor coordination. These muscles are precision sensors, not power movers.
That position information drives reflexes that set muscle tone far beyond the neck. The cervical afferents feed several major reflex pathways — including the cervico-collic reflex and the tonic neck reflex — that translate head-and-neck position into coordinated, whole-body muscle activation. Experimental work confirms the system's reach: intact neck neuromuscular function is required to maintain normal standing posture, and disturbing neck proprioception measurably degrades balance and postural control. The upper neck is, quite literally, wired to dictate how your postural muscles behave.
The core idea: The atlas (C1) sits at the top of the postural control system. If it's misaligned and sending faulty position signals, the reflexes that set muscle tone can hold your head forward and flatten your cervical curve — and keep them that way no matter how often you try to "sit up straight."
How an atlas misalignment pulls the head forward or reverses the curve
The atlas is the topmost vertebra, the ring that the skull rests on. It governs an outsized share of neck motion — the upper cervical spine (C0–C2) is responsible for roughly 50% of total neck flexion and extension and 50% of overall cervical rotation. Because so much movement and so much sensory input concentrate here, a small misalignment at the atlas has effects out of all proportion to its size.
When the atlas shifts out of its normal position, two things happen. First, the high-density sensors there begin reporting distorted head-position information, and the reflex system responds by changing muscle tone throughout the postural chain. Second, the body must level the eyes and inner ear regardless of what the atlas is doing, so it compensates lower down. The documented pattern of forward head posture involves exactly this: increased extension of the upper cervical vertebrae and the occiput on C1, with increased flexion of the lower cervical and upper thoracic regions. In plain terms — the top of the neck tips back, and the rest of the neck flexes forward to compensate, flattening or reversing the curve.
This is the atlas-to-kyphosis link. An atlas misalignment alters the tone-setting signals, the head is carried forward of its balance point, and the lower cervical spine loses its lordosis to keep the eyes level. The curve doesn't flatten on its own — it's pulled flat by a postural control system responding to a faulty signal at the very top.
The compensation chain: upper-crossed syndrome
Clinically, this whole pattern has a name: upper-crossed syndrome, described by the physician Vladimir Janda. It refers to a predictable imbalance in which certain muscles become tight and overactive (the suboccipitals, upper trapezius, levator scapulae, pectorals, and sternocleidomastoid) while their opposites become weak and inhibited (the deep neck flexors, rhomboids, and lower trapezius). This crossed pattern produces forward head posture, rounded and protracted shoulders, and increased thoracic kyphosis.
The curves are linked together in a chain reaction. As one clinical description puts it, the greater the thoracic kyphosis, the greater the lower cervical hypolordosis and the greater the upper cervical hyperlordosis — the upper cervical extensors tighten and pull the top of the neck into extension to bring the eyes level, compensating for the flattening below. Each segment's distortion drives the next. This is why cervical kyphosis is rarely an isolated finding: it travels with rounded shoulders, a hunched upper back, and a head carried forward, all locked together by muscle tone the upper neck helps govern.
Symptom #1:
Arm numbness and tingling — scalene entrapment of the brachial plexus
One of the most alarming consequences of cervical kyphosis and forward head carriage is numbness, tingling, and aching that travels down the arm into the hand. The mechanism runs straight through the neck.
The brachial plexus — the bundle of nerves supplying the arm — exits the cervical spine and passes through a narrow triangle formed by the scalene muscles of the neck and the first rib. The scalenes originate from the cervical vertebrae, so their tension is governed by cervical posture and tone. When the head is carried forward and the scalenes are chronically shortened and overworked to hold it up, that triangle narrows and the nerve bundle gets compressed — a pattern closely related to thoracic outlet syndrome. Symptom surveys of upper-crossed syndrome and forward head posture consistently include numbness and tingling in the upper arms among the commonly reported symptoms.
This is the same control-system story applied to the nerve. The scalenes that pinch the brachial plexus are downstream; the upper neck that sets their tone is upstream. If an atlas misalignment is holding the head forward and keeping the scalenes engaged, stretching them alone tends to give only temporary relief, because the reflex system keeps re-tightening them. The arm symptoms are a signal pointing back up the neck.
Symptom #2:
Mid-thoracic and upper-back pain — the cost of forward head carriage
Mid-back and upper-back pain between the shoulder blades is one of the most common complaints that travels with cervical kyphosis — and it's a direct mechanical consequence of carrying the head forward.
When the head drifts ahead of the shoulders, its effective load on the spine increases dramatically, and the muscles of the upper back and the cervicothoracic junction must work continuously to keep you from pitching forward. The body deepens the thoracic kyphosis to compensate, and the postural muscles between the shoulder blades fatigue under the constant strain. Forward head posture is well documented to affect not only the neck but also the thoracic spine and shoulder blade, producing overall imbalance across the musculoskeletal system. The upper-crossed pattern likewise lists upper-back pain and chest tightness among its hallmark symptoms.
Notably, the thoracic spine is sometimes called a "silent saboteur" — the kyphotic upper back drags the lower neck into flexion, and the neck follows the curve of the upper back into forward carriage. The mid-thoracic pain and the cervical kyphosis aren't two separate problems; they're two ends of the same postural chain, with muscle tone — governed in significant part from the upper neck — holding the whole pattern in place.
Other associated symptoms
Because the upper neck integrates with the visual and vestibular systems and governs postural tone, cervical kyphosis and its forward-head pattern are associated with a wider cluster of complaints than most people realize. Commonly reported associations include tension-type and cervicogenic headaches (from the chronically tightened suboccipital and upper trapezius muscles), neck pain and stiffness, restricted neck and shoulder range of motion, jaw and TMJ discomfort, dizziness and balance complaints (cervicogenic dizziness), and reduced breathing efficiency from a collapsed-forward chest posture. Research on forward head posture notes it can contribute to a multitude of disorders including cervical radiculopathy, cervicogenic headaches, and cervicogenic dizziness, often presenting as clusters of symptoms rather than a single complaint. The unifying thread is the same: a postural control system, anchored at the top of the neck, that has been pulled out of balance.
The myodural bridge and the proprioceptive loop
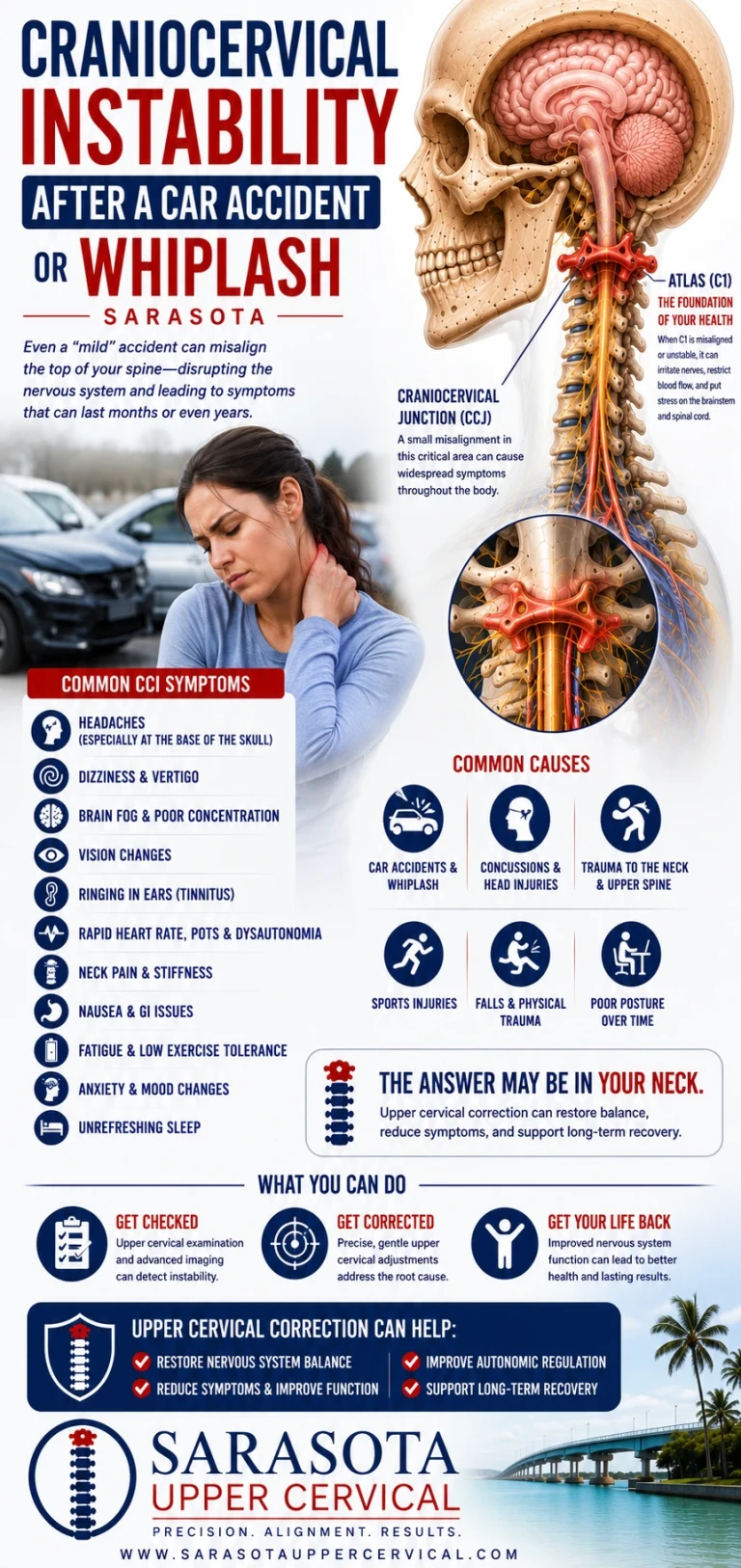
Two final mechanisms explain why this pattern becomes self-sustaining. The first is the myodural bridge , a band of connective tissue physically connecting the deep suboccipital muscles, chiefly the rectus capitis posterior minor, to the dura mater that surrounds the spinal cord. Whiplash-type injuries transmit traction forces through this bridge to the cervical dura, which is one reason a past neck injury can leave a lasting imprint on upper cervical function and posture.
The second is the proprioceptive feedback loop. Once an atlas misalignment distorts the position signals, the reflex system raises postural muscle tone and carries the head forward; the forward head flattens the curve and keeps the suboccipitals and scalenes tight; and the resulting dysfunction feeds still more distorted signals back into the system. Research shows the tight coupling directly: higher tone in the suboccipital muscles is significantly associated with a more forward head posture. The faulty signal and the faulty posture reinforce each other — which is precisely why kyphosis and forward head carriage are so persistent, and why addressing the top of the chain matters.
The upper cervical approach in Sarasota — and its limits
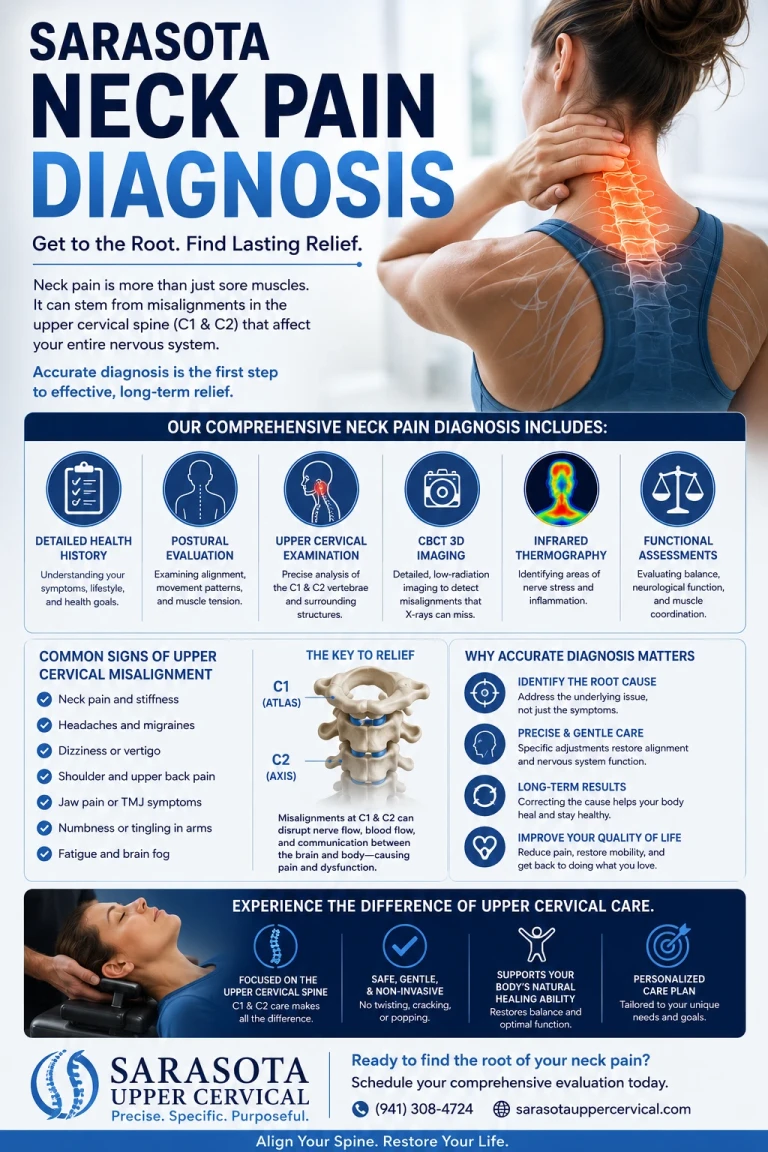
Upper cervical chiropractic care focuses on the alignment and motion of the atlas (C1) and axis (C2), because that's the control point for the proprioceptive and reflex system that governs postural muscle tone. The goal isn't to force the neck or chase a feeling — it's to restore normal position and motion at the top of the cervical spine so the sensors there report accurately again, allowing the reflex-driven postural tone, head carriage, and cervical curve to normalize from the top down. There's measurable support for the upstream effect: a randomized controlled trial found that upper cervical manipulation produced significant improvement in global postural-control measures, reducing standing-balance sway velocity, surface area, and path length — direct evidence that the top of the neck moves whole-body postural control.
Related article

Tinnitus Relief: Understanding the Upper Cervical Connection to Ear Ringing
Jan 26, 2026Why CBCT imaging matters
Because the correction is precise, the analysis must be precise. At Sarasota Upper Cervical we use cone beam computed tomography (CBCT) as a precision measurement tool — it reveals the true three-dimensional position of the atlas and axis far more accurately than a flat 2D X-ray. The misalignments that drive postural tone are often just a few degrees of rotation or a small lateral shift, and the head carriage and curve respond to exactly that kind of subtle positioning. CBCT lets us measure it in three dimensions and tailor the analysis to your individual anatomy rather than guessing. (CBCT is a measurement and analysis tool, not a stand-alone diagnostic device for kyphosis; the structural assessment is clinical and radiographic.)
The honest boundaries
Not all cervical kyphosis is postural. Some is structural or congenital, some follows fracture, surgery, or advanced degenerative disease, and some is driven by conditions that need medical or surgical management. Progressive numbness, weakness, hand clumsiness, or loss of coordination are red flags that warrant prompt neurological evaluation. Upper cervical care is a complement to appropriate medical assessment, not a replacement for it — a thorough upper cervical doctor will help identify whether your case has a postural-mechanical driver worth addressing, and will refer out when it doesn't.
Questions and Answers
How can the atlas at the top of my neck cause my curve to flatten lower down?
The atlas doesn't flatten the curve directly — it controls the muscle tone that holds your head and neck in position. When the atlas is misaligned, it sends distorted position signals, the reflex system pulls the head forward of its balance point, and the lower cervical spine flexes to keep your eyes level. That compensation is what flattens or reverses the curve. The top of the neck tips back; the rest follows forward.
Why do I have numbness and tingling in my arm with a neck problem?
The nerves that supply your arm (the brachial plexus) pass through a narrow triangle formed by the scalene muscles of the neck and the first rib. When forward head carriage keeps those scalenes shortened and tight, the triangle narrows and the nerves get compressed, producing numbness, tingling, and aching down the arm. Because the scalenes' tone is set by cervical posture, addressing the upper neck addresses the upstream driver.
Why does my mid-back hurt if the problem is in my neck?
Carrying the head forward dramatically increases its load on the spine, forcing the upper-back muscles between the shoulder blades to work constantly and deepening the thoracic kyphosis. The mid-back pain and the cervical kyphosis are two ends of the same postural chain — the kyphotic upper back and the forward head pull on each other, held together by muscle tone the upper neck helps govern.
I've tried stretching and ergonomic changes. Why hasn't my posture improved?
Because stretching and ergonomics address the bottom of the pattern while the control system at the top keeps driving it. If the atlas is misaligned and the reflexes are holding your postural muscles in a tightened, head-forward state, those muscles tend to return to that state after you stretch. Normalizing the upstream signal is what gives the postural tone a chance to reset and hold.
Is all cervical kyphosis treatable this way?
No. Some kyphosis is structural, congenital, or the result of fracture, surgery, or advanced degeneration, and those forms require medical or surgical management. Upper cervical care addresses the postural-mechanical contributors. Progressive weakness, numbness, hand clumsiness, or coordination loss are red flags that need prompt medical evaluation. A good upper cervical doctor will help determine which type you have and refer out when appropriate.
Why CBCT instead of a regular X-ray?
CBCT shows the true three-dimensional position of the atlas and axis, where a flat X-ray captures only two dimensions. The misalignments that drive postural tone are often a few degrees of rotation or a small shift, and seeing them accurately allows a precise, individualized analysis. We use it as a measurement and analysis tool; the structural assessment of the curve itself remains clinical and radiographic.
Kyphosis treatment and relief in Sarasota
If you have a flattening or reversed neck curve, forward head posture, mid-back pain, or arm numbness and tingling that hasn't resolved, a focused upper cervical evaluation can help determine whether the root driver is at the top of your neck — working alongside your medical care.
This article is for general educational purposes only and is not medical advice, a diagnosis, or a treatment recommendation for any individual. Cervical kyphosis can have postural, structural, congenital, traumatic, degenerative, or other causes; structural and progressive cases require medical or surgical evaluation, and upper cervical chiropractic care is intended to address postural and mechanical contributors as a complement to appropriate medical care, not as a cure or a replacement for it. Upper cervical chiropractic is an area of focus within chiropractic; it is not a board-recognized specialty, and no claim of specialization or superiority is made or implied. Cone beam CT is used as a precision measurement and analysis tool, not as a stand-alone diagnostic device. The mechanisms and research described are presented for education; individual results vary, and no specific outcome is guaranteed. Always consult a qualified healthcare provider regarding diagnosis and treatment of cervical kyphosis or any neurological symptoms such as progressive numbness, weakness, or loss of coordination.



Leave a comment