
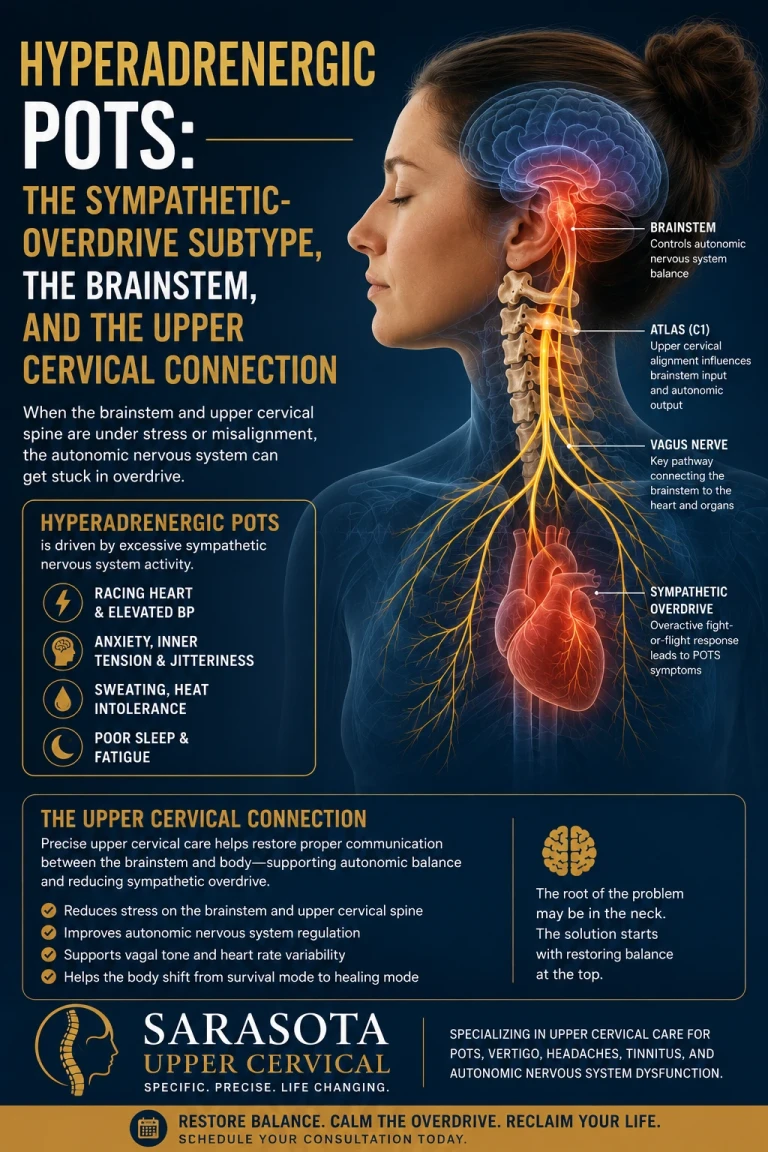
If your POTS comes with pounding palpitations, tremor, surges of flushing and adrenaline, high blood pressure when you stand, and an anxiety that feels physical rather than emotional, you may have the hyperadrenergic subtype. It's the version of POTS most often mistaken for an anxiety disorder, and the one where the phrase "stuck in fight-or-flight" is closest to literally true. Understanding why your nervous system is stuck in overdrive — and where the upper neck fits into that overdrive, can change how you approach getting relief.
This article looks at hyperadrenergic POTS through the lens of the nervous system that drives it: the sympathetic "fight-or-flight" branch, the brainstem control centers that regulate it, and the upper cervical spine that surrounds and protects those centers. One boundary up front: POTS is a serious medical condition requiring physician diagnosis and management, and upper cervical chiropractic does not cure POTS or any subtype. What it focuses on is one possible contributor to autonomic balance, the mechanical environment of the brainstem at the top of the neck.
Schedule Your Appointment
Schedule appointmentWhat hyperadrenergic POTS is
POTS (postural orthostatic tachycardia syndrome) is the most common form of dysautonomia, a malfunction in the autonomic nervous system that shows up as a racing heart, lightheadedness, and a cluster of other symptoms when you stand. Clinicians sometimes describe subtypes to help think about the underlying mechanism, and the hyperadrenergic subtype is the "too much sympathetic activity" version. It is one of the most common forms, comprising up to roughly 50% of POTS patients, and is thought to involve elevated norepinephrine driven in part by a defect in the norepinephrine transporter, the molecule that normally clears the "fight-or-flight" neurotransmitter from the nerve synapse.
The distinguishing features matter, because they're what separate it from the other subtypes: excessive tachycardia on standing, a rise in systolic blood pressure of more than 10 mmHg, and elevated standing norepinephrine levels of 600 pg/mL or more, along with palpitations, sweating, nausea, and tremor. Where most POTS subtypes involve blood pressure that stays flat or drops on standing, hyperadrenergic POTS often shows blood pressure that climbs, a key clinical fingerprint of sympathetic overdrive.
An important honesty note: The POTS "subtypes" are a useful framework, not rigid boxes. Clinicians don't all use them, they overlap heavily, and one person can fit more than one. Hyperadrenergic features frequently coexist with neuropathic or hypovolemic mechanisms. Treat this as a lens for understanding your nervous system, not a fixed diagnostic label, and let your physician determine what actually applies to you.
Why it gets misdiagnosed as anxiety
This is the part that sends so many hyperadrenergic POTS patients on a years-long detour. The symptoms of sympathetic overdrive, racing heart, tremor, sweating, flushing, a sense of dread or panic, are physiologically almost identical to a panic attack. The difference is the driver: in hyperadrenergic POTS, the "adrenaline" state is coming from a dysregulated autonomic nervous system, often triggered by standing or exertion, not from a primary psychological cause.
The clinical literature is blunt about this trap: hyperadrenergic POTS can be especially challenging because symptoms overlap with anxiety, and patients are sometimes prescribed medications that may worsen symptoms if the root issue isn't addressed. That last point is critical, some anxiety medications (particularly those that raise norepinephrine, like SNRIs) can make hyperadrenergic POTS worse. Being told "it's just anxiety" isn't only invalidating; it can lead to treatment that backfires. The physical adrenaline surges are real, measurable events, not a mindset.
Related article
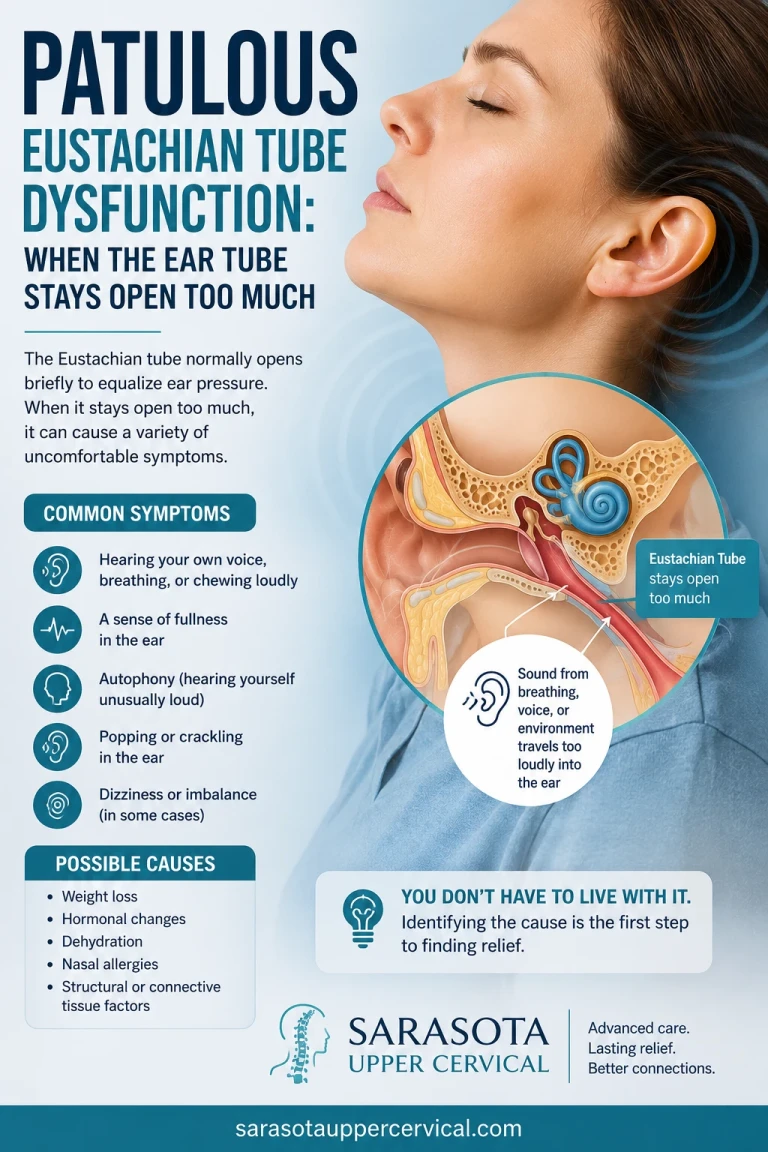
Patulous Eustachian Tube Dysfunction: When the Ear Tube Stays Open Too Much
May 26, 2026The brainstem: where sympathetic drive is actually regulated
To see where the upper neck fits, you have to know where the "fight-or-flight" dial physically lives. It's in the brainstem — specifically the medulla, at the base of the skull. The master control center for sympathetic outflow is a region called the rostral ventrolateral medulla (RVLM), and it does exactly the job hyperadrenergic POTS gets wrong. The RVLM is the "pressor area" of the medulla, responsible for basal and reflex control of sympathetic activity for cardiovascular function, and it is central to the baroreflex — the reflex that adjusts heart rate and blood pressure when you change position. It provides tonic, moment-to-moment sympathetic drive to the heart and blood vessels, including a group of epinephrine-containing neurons that set the baseline.
Sitting right beside it are the parasympathetic and sensory nuclei, the nucleus tractus solitarius (which receives the body's blood-pressure and inflammatory reports) and the dorsal motor nucleus of the vagus (which sends the parasympathetic "brake" back out via the vagus nerve). This tight cluster of brainstem nuclei is the physical hardware of autonomic balance: the sympathetic accelerator and the vagal brake, side by side. And a recent mechanistic review notes that these key autonomic structures, the nucleus tractus solitarius, the dorsal motor nucleus of the vagus, and the rostral ventrolateral medulla, reside within the medulla and are precisely where orthostatic-intolerance and POTS-like phenotypes can arise from craniocervical-junction disorders.
Here's the crux: all of this hardware sits inside the craniocervical junction, the space enclosed by the base of the skull and the top two vertebrae of the neck, the atlas (C1) and axis (C2). The brainstem's autonomic control room is housed at the very top of your neck.
The atlas, brainstem irritation, and faulty proprioceptive input
This is where the upper cervical connection becomes specific and mechanical, not a vague "everything's connected" claim, but documented neuroanatomy.
The upper cervical spine is the most proprioceptively dense region of the entire body. Its small muscles and joints are packed with position sensors, and, critically, those sensors don't just feed posture and balance. They feed the autonomic system. Research tracing upper cervical sensory nerves found that stimulating the second cervical nerve altered central respiratory drive and increased perfusion pressure, and revealed a short-latency response in sympathetic nerve activity, with the responsible fibers identified as proprioceptive. In plain terms: proprioceptive signals from the upper neck project directly into the medulla and can change sympathetic output. There is a documented network of neurophysiological connections between the cervical spine mechanoreceptors and the sympathetic nervous system.
Now consider what happens when that input goes bad. When the atlas is misaligned and the upper cervical joints lose normal motion, commonly after whiplash, concussion, or head/neck trauma, the proprioceptive signal becomes distorted. As one review describes, in chronic cervical dysfunction the mechanoreceptors are compromised and the cervical afferents transmit impaired proprioceptive signals, with these patients often having a history of neck pain, whiplash, or concussion. The nervous system is now receiving a faulty position report from the very region that houses the sympathetic control center, and feeding it into the medulla that sets sympathetic tone.
Related article
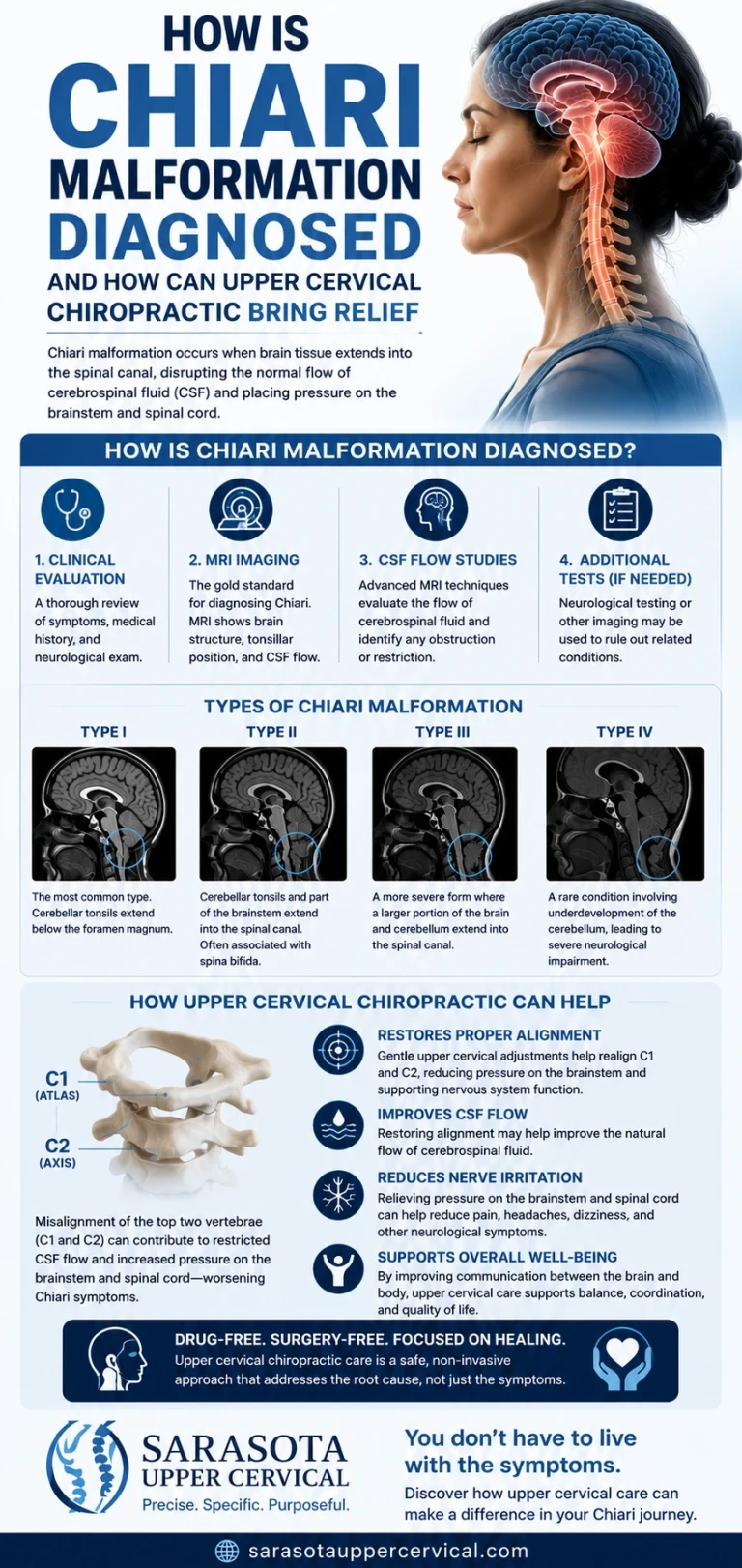
How is chiari malformation diagnosed and how can upper cervical chiropractic bring relief
Jul 12, 2026The proposed consequence: distorted upper cervical proprioceptive input, plus mechanical irritation of the brainstem environment at the craniocervical junction, may nudge an already-dysregulated autonomic system further toward sympathetic dominance, the exact overdrive state that defines hyperadrenergic POTS. This is a real, documented association in related conditions: cervical dystonia patients (who have profoundly disturbed neck posture and afferent input) show measurable autonomic dysfunction reflecting abnormal parasympathetic-sympathetic interaction, likely related to abnormal neck posture. Disturbed neck input and autonomic imbalance travel together.
The thermostat analogy: Think of the brainstem as the thermostat regulating your autonomic "temperature." The upper cervical proprioceptors are part of the sensor feeding that thermostat. When the atlas is misaligned, it's like draping a towel over the sensor, the thermostat starts getting faulty readings and can crank the sympathetic "heat" when it shouldn't. The control center is intact; the input and output are distorted.
Where upper cervical care fits, honestly
What upper cervical care can reasonably focus on is autonomic balance: restoring normal alignment and proprioceptive input at the craniocervical junction, so the brainstem stops receiving a distorted position signal and one source of mechanical interference is removed from the system that regulates sympathetic and parasympathetic tone. The rationale is that the upper cervical spine surrounds and protects the brainstem, and when the atlas or axis becomes even slightly misaligned it can alter the environment around the brainstem, with care focused on improving the body's ability to self-regulate rather than addressing symptoms individually. For a hyperadrenergic POTS patient with a history of head or neck trauma, that's a reasonable, low-risk avenue to evaluate.
It's worth distinguishing this from craniocervical instability (CCI), a more severe ligamentous laxity seen in some hypermobile/EDS patients that is strongly associated with POTS and is sometimes managed surgically. That is a different and more serious problem than the upper cervical misalignment upper cervical chiropractic addresses, and suspected CCI warrants specialized medical evaluation. The shared theme across both is simply that the craniocervical junction matters for autonomic function.
Why CBCT imaging matters here
Because any upper cervical correction is precise, the analysis must be precise. We use cone beam computed tomography (CBCT) as a precision measurement tool to see the true three-dimensional position of the atlas and axis, so an assessment is tailored to the individual's anatomy rather than estimated. (CBCT is a measurement and analysis tool; it is not a diagnostic test for POTS, which is diagnosed clinically with standing or tilt-table testing.)
What the broader research suggests
The idea that supporting autonomic regulation helps dysautonomia is supported from several directions. A randomized controlled trial found that cervical lordosis rehabilitation produced measurable changes in autonomic nervous function and cervical sensorimotor control, and case reports describe conservative cervical care helping POTS-associated presentations, sometimes on referral from cardiologists after structural heart causes were ruled out. This research is still emerging and much of it is preliminary,it establishes plausibility and direction, not proof of cure. But it points consistently at the same target: the nervous system's ability to self-regulate, which is exactly what the upper cervical approach aims to support.
Questions and Answers
Is hyperadrenergic POTS just anxiety?
No. The symptoms overlap heavily with anxiety, racing heart, tremor, sweating, a sense of dread, but in hyperadrenergic POTS these are driven by a dysregulated autonomic nervous system with measurably elevated norepinephrine, often triggered by standing. It's a physical, measurable state, not a primarily psychological one. This distinction matters because some anxiety medications that raise norepinephrine can actually worsen hyperadrenergic POTS, which is why an accurate diagnosis is so important.
Can upper cervical chiropractic cure my hyperadrenergic POTS?
What upper cervical focuses on is autonomic balance — restoring normal alignment and proprioceptive input at the craniocervical junction where the brainstem's autonomic control centers sit, to remove one possible source of mechanical interference. It's a complement to medical care, especially for patients with a history of head or neck trauma, not a replacement or a cure. With that said many POTS patients find significant relief and a better aulity of life under upper cervcial corrective care.
How does the atlas affect my "fight-or-flight" system?
The brainstem region that sets sympathetic (fight-or-flight) drive, the rostral ventrolateral medulla, sits inside the craniocervical junction, enclosed by the skull and the atlas and axis. The upper neck is also the body's most proprioceptively dense region, and its position sensors project into the medulla and can influence sympathetic output. When the atlas is misaligned, that input becomes distorted, which may nudge an already-dysregulated system further toward sympathetic overdrive.
Are the POTS subtypes definite categories?
No. The subtypes, hyperadrenergic, neuropathic, hypovolemic — are a useful framework for thinking about mechanisms, but they're not universally used, they overlap substantially, and one person can fit more than one. They're best treated as a lens for understanding your nervous system rather than fixed diagnostic boxes. Your physician determines what actually applies to you.
What's the difference between upper cervical misalignment and craniocervical instability?
Upper cervical misalignment refers to the position and motion of the atlas and axis that upper cervical chiropractic addresses. Craniocervical instability (CCI) is a more severe ligamentous laxity, seen more often in hypermobile or Ehlers-Danlos patients, that is strongly associated with POTS and is sometimes managed surgically. They're different in severity and management, and suspected CCI needs specialized medical evaluation. The common thread is that the craniocervical junction matters for autonomic function.
Hyperadrenergic POTS and the upper cervical connection | Sarasota
If your POTS runs in the "sympathetic overdrive" direction — palpitations, tremor, adrenaline surges, high standing blood pressure — especially after a head or neck injury, a focused upper cervical evaluation can help determine whether the mechanical environment of your brainstem is worth addressing alongside your medical care.
This article is for general educational purposes only and is not medical advice, a diagnosis, or a treatment recommendation for any individual. POTS and hyperadrenergic POTS are serious medical conditions that must be diagnosed and managed by qualified physicians. Upper cervical chiropractic does not cure POTS or any subtype and is not a substitute for medical care; it focuses on mechanical and proprioceptive contributors at the craniocervical junction that may influence autonomic balance, as a complement to appropriate medical management. Upper cervical chiropractic is an area of focus within chiropractic; it is not a board-recognized specialty, and no claim of specialization or superiority is made or implied. The POTS subtype framework is a non-definitive clinical model with substantial overlap between subtypes. Cone beam CT is used as a precision measurement and analysis tool, not as a diagnostic device for POTS. The mechanisms and research described — including craniocervical-junction associations, cervical proprioceptive influences on autonomic function, and cervical rehabilitation studies — are emerging, in many cases preliminary, and are presented for education rather than as proof of treatment outcomes. Individual results vary, and no specific outcome is guaranteed. Seek prompt medical attention for chest pain, fainting, severe blood-pressure or heart-rate changes, or new or worsening symptoms. Always consult your physician regarding diagnosis and management of POTS.



Leave a comment