
Ear fullness. Clicking and popping. Pressure in front of the ear. Muffled or altered hearing. These symptoms sit right at the overlap between two conditions that are constantly confused for each other — eustachian tube dysfunction (ETD) and temporomandibular joint disorder (TMJ/TMD). Many people spend months being treated for one when the other is driving it, or never realize both are being fed by a third factor upstream: the upper cervical spine.
This article breaks down how to tell ETD and TMJ apart, why they overlap so heavily, and, most importantly — the neurological connection at the base of the skull that links the jaw, the ear, and the neck into a single system. That upper cervical link is the part most ear and jaw evaluations leave out entirely.
Schedule Your Appointment
Schedule appointmentWhy these two get confused
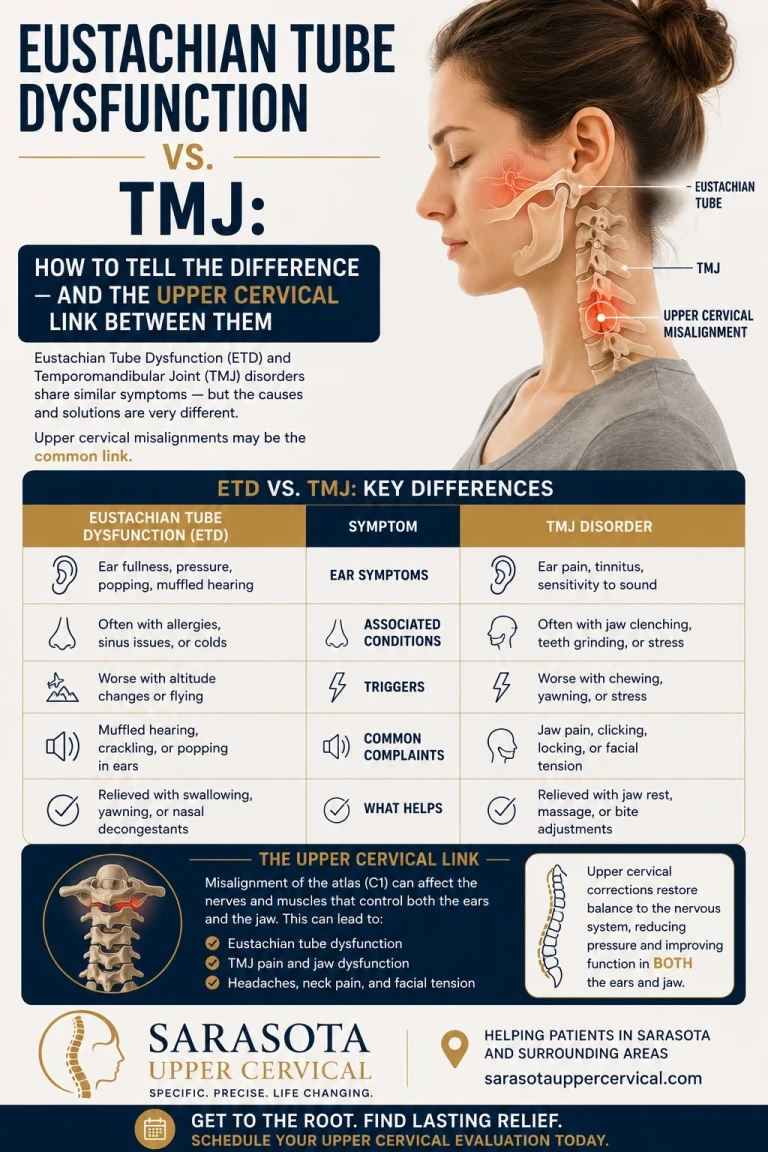
The confusion is anatomical: the temporomandibular joint sits directly in front of the ear canal, millimeters from the eustachian tube and the muscles that open it. When that joint and its muscles are dysfunctional, the symptoms show up in the ear. The diagnostic literature recognizes TMJ as a direct ETD mimic, patients with TMJ dysfunction describe discomfort in front of and around the ear, typically on one side, sometimes with clicking or popping noises and altered hearing or tinnitus. The cardinal clue, per the same consensus statement, is that jaw-related TMJ pain is aggravated by manipulation or function of the jaw, chewing, talking, yawning.
And the two genuinely co-occur. Because the jaw and middle ear share some nerves and muscles, a jaw condition can affect the eustachian tube itself — so this isn't always an either/or. Sometimes TMJ dysfunction is actively producing the ear symptoms.
How to tell them apart
No article replaces a proper exam, but here's how the two patterns typically differ:
A rough rule of thumb: if your ear symptoms flare when you chew, talk, or yawn, or you have jaw clicking, locking, or tenderness, TMJ deserves a hard look. If they flare with colds, allergies, or altitude and there's no jaw component, ETD is the better fit. When both sets of clues are present, that's a signal to look upstream — which is where the upper cervical spine enters.
Related article
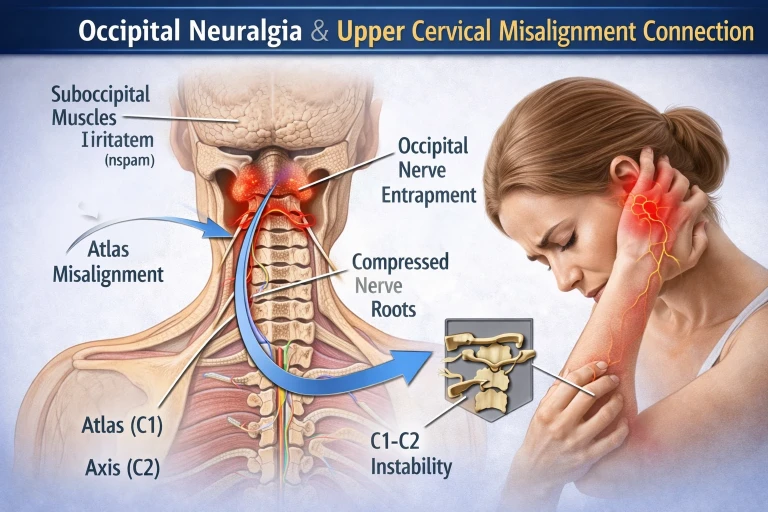
Sharp Pain at the Base of the Skull? | Lakewood Ranch Upper Cervical Care |Occipital Neuralgia
Mar 05, 2026The upper cervical link: one nucleus connecting neck, jaw, and ear
Here is the connection that reframes the whole ETD-vs-TMJ question. The jaw and the upper neck are not separate neurological territories — they share a single processing hub in the brainstem called the trigeminocervical nucleus.
The sensory nerve that supplies the TMJ (the trigeminal nerve, cranial nerve V), the motor nerves that move the jaw muscles, and the sensory nerves of the upper neck (the C1, C2, and C3 nerve roots) all converge and communicate in a shared region called the trigeminocervical nucleus. The functional consequence is direct: upper cervical spine problems involving the C1–C3 nerve roots can influence the motor nerves that control the muscles crossing the TMJ — including the same muscles (the pterygoids) that are intimately related to the muscle that opens the eustachian tube.
This is why the upper neck is the common denominator. A misalignment or dysfunction at the top of the cervical spine feeds aberrant input into the trigeminocervical nucleus, which can drive abnormal jaw-muscle tone (a TMJ presentation) and, through the shared muscular and fascial relationships around the tube, contribute to faulty eustachian tube opening (an ETD presentation). One upstream problem, two downstream faces.
The key concept: ETD and TMJ aren't just neighbors that get confused — they're wired into the same brainstem hub as the upper cervical spine. When the neck sends faulty signals into that hub, it can show up as jaw dysfunction, ear dysfunction, or both. Treating only the ear or only the jaw can miss the driver feeding both.
The research behind the upper cervical connection
This isn't just a mechanistic story — there's measurable evidence the upper neck influences the jaw. A 2023 systematic review and meta-analysis examined upper cervical mobilization and manipulation for TMJ disorders and grounded the approach in exactly this anatomy, noting that the complex biomechanical, anatomical, and neurophysiological links between the upper cervical spine and the trigeminal nucleus provide a clinical basis for treating the cervical spine in TMJ dysfunction.
The posture and proprioception data point the same way. A case-control study found that people with myogenic (muscle-driven) TMD have measurably worse cervical joint position sense — the neck's ability to accurately sense its own position — than healthy individuals, with cervical and jaw disability significantly correlated. And a 2025 systematic review on jaw-and-neck mechanics reported that maximal mouth opening was greatest in forward head posture compared with neutral or retracted positions, with trigeminal nociceptive processing shifting across different craniocervical postures — direct evidence that where the head sits on the neck changes how the jaw functions and processes pain. Reviews of craniocervical alignment go further, suggesting that abnormalities in craniocervical alignment, including incorrect alignment of the C1 and C2 vertebrae, may contribute to the development and progression of TMJ dysfunction.

Taken together: the upper cervical spine measurably influences jaw mechanics, jaw pain processing, and the proprioceptive signaling that keeps both systems calibrated. For a patient whose ear and jaw symptoms keep cycling despite ear-only or jaw-only treatment, that upstream influence is the missing variable.
Where upper cervical care fits
Upper cervical chiropractic care focuses on the alignment and motion of the atlas (C1) and axis (C2) — the precise region feeding the trigeminocervical nucleus. The goal isn't to "treat the ear" or "treat the jaw" directly; it's to restore normal input from the top of the neck so the shared hub stops receiving faulty signals, allowing jaw-muscle tone, head posture, and the muscular environment around the eustachian tube to normalize. For the patient caught between an ETD diagnosis and a TMJ diagnosis — especially after whiplash, a blow to the head or jaw, or with chronic forward-head posture — addressing the upper cervical contributor targets the one factor that sits upstream of both.
Why CBCT imaging matters here
Because the upper cervical correction is precise, the analysis must be precise. We use cone beam computed tomography (CBCT) as a precision measurement tool to see the true three-dimensional position of the atlas and axis. Notably, CBCT is increasingly used to study this very relationship: research has used it to correlate degenerative changes between the TMJ and the upper cervical vertebrae, reflecting how interconnected these structures are. For our purposes, CBCT measures the upper cervical misalignment in three dimensions so the analysis is tailored to your individual anatomy rather than estimated. (CBCT is a measurement and analysis tool; diagnosis of ETD or TMJ is clinical.)
The smart sequence if you're stuck between the two
If you've been bounced between "it's your ears" and "it's your jaw" without lasting relief, a sensible path is: get a proper ENT and/or dental-TMJ evaluation to confirm the diagnosis and rule out red flags; treat the obvious drivers (allergy, sinus, reflux for ETD; bite, clenching, bruxism for TMJ); and have the upper cervical spine evaluated as the shared upstream contributor — particularly if there's a history of head or neck trauma or persistent forward-head posture. Addressing the common denominator is often what finally breaks the cycle when single-system treatment hasn't.
When to seek prompt evaluation
Some symptoms shouldn't wait. Seek timely medical care for sudden hearing loss, severe or worsening ear or facial pain, fluid or blood draining from the ear, a jaw that locks open or closed, persistent dizziness or vertigo, or symptoms following significant head or jaw trauma. Persistent ear or jaw symptoms beyond two to three weeks warrant a provider visit rather than indefinite self-management.
Questions and Answers

How do I know if my ear fullness is from ETD or TMJ?
A useful first test is what triggers it. If your ear symptoms flare when you chew, talk, or yawn, or you also have jaw clicking, locking, or tenderness, TMJ deserves a close look. If they flare with colds, allergies, or altitude changes like flying — with no jaw component — eustachian tube dysfunction is the better fit. When both patterns are present, it points to a shared upstream contributor like the upper cervical spine, and a proper exam is needed to sort it out.
Can TMJ actually cause eustachian tube dysfunction?
It can contribute. The jaw joint sits directly in front of the eustachian tube and shares nerves and muscles with the middle-ear region, so jaw dysfunction can affect how the eustachian tube opens and functions. This is one reason the two conditions overlap and are frequently confused, and why evaluating both — along with the upper neck that influences both — often makes sense.
What does the neck have to do with my jaw and ear symptoms?
The jaw's sensory and motor nerves and the upper neck's C1–C3 nerve roots all converge in a shared brainstem hub called the trigeminocervical nucleus. Faulty input from an upper cervical misalignment can feed that hub and contribute to abnormal jaw-muscle tone and altered function around the eustachian tube — meaning one upstream neck problem can show up as jaw dysfunction, ear dysfunction, or both.
Is there research linking the upper cervical spine to TMJ?
Yes. A 2023 systematic review and meta-analysis examined upper cervical mobilization and manipulation for TMJ disorders, grounded in the anatomical and neurophysiological links between the upper cervical spine and the trigeminal nucleus. Other studies show people with TMJ disorders have worse cervical joint position sense, and that head posture measurably affects mouth opening and jaw pain processing. Reviews also suggest C1–C2 alignment may influence TMJ dysfunction.
I've been treated for both my ears and my jaw with no lasting relief. Why?
When ear-only or jaw-only treatment keeps falling short, it can be because both are downstream of a shared contributor that wasn't addressed. The upper cervical spine feeds the same neurological hub as the jaw and influences the muscular environment around the eustachian tube. Evaluating and addressing that common denominator — alongside your ENT and dental care — is often what's missing when single-system treatment hasn't worked.
When should I see a doctor right away?
Seek prompt care for sudden hearing loss, severe or worsening ear or facial pain, fluid or blood draining from the ear, a jaw that locks open or closed, persistent dizziness or vertigo, or symptoms after significant head or jaw trauma. Persistent ear or jaw symptoms beyond two to three weeks also warrant a provider visit.
Caught between an ear and a jaw diagnosis? Sarasota upper cervical care
If your ear fullness and jaw symptoms keep cycling despite treatment — especially after head or neck trauma — a focused upper cervical evaluation can help determine whether the upstream contributor feeding both has been missed, working alongside your ENT and dental care.
This article is for general educational purposes only and is not medical advice, a diagnosis, or a treatment recommendation for any individual. Eustachian tube dysfunction and temporomandibular joint disorders should be evaluated by qualified medical, ENT, or dental providers. Upper cervical chiropractic is an area of focus within chiropractic; it is not a board-recognized specialty, no claim of specialization or superiority is made or implied, and it addresses mechanical and postural contributors as a complement to appropriate medical and dental care rather than a replacement for it. Cone beam CT is used as a precision measurement and analysis tool, not as a stand-alone diagnostic device. The mechanisms and research described are presented for education; individual results vary, and no specific outcome is guaranteed. Seek prompt medical attention for sudden hearing loss, severe pain, ear drainage, a locked jaw, persistent dizziness, or symptoms following trauma. Always consult a qualified healthcare provider regarding diagnosis and treatment.



Leave a comment