
The same impact that concusses the brain also injures the neck — and for the many people whose symptoms never fully resolve, an unexamined upper-neck injury may be the reason recovery has stalled.
Sarasota Upper Cervical · Post-Concussion Care Serving Sarasota Lakewood Ranch - Bradenton-Venice -Englewood -Northport
Schedule Your Appointment
Schedule appointmentWhat this guide covers
1.When a concussion doesn't heal on schedule
2.One impact, two injuries
3.Why the neck injury gets missed
4.How an upper-neck injury interferes with the nervous system
5.The full symptom picture of PCS
6.Why the symptom overlap matters
7.Why clearing the upper neck matters for recovery
8.Where upper cervical care fits
9.What it does and doesn't do
10.Our approach in Sarasota
11.FAQ
When a concussion doesn't heal on schedule
Most concussions get better. With relative rest and a gradual return to activity, the large majority of people recover within a few weeks, and the standard advice works exactly as advertised. But there's a group for whom it doesn't — people who are still struggling months or even years later with headaches, brain fog, dizziness, fatigue, and a long list of other symptoms, long after they were told they'd be "back to normal." When symptoms persist past the expected window, it's called post-concussion syndrome (PCS), or persistent post-concussion symptoms.
Here's the question that should be asked far more often: if rest resolves the overwhelming majority of concussions but does nothing for these lingering cases, is it possible that the persistent symptoms aren't coming entirely from the brain? A growing body of evidence says yes — and points to a structure that standard concussion care almost never examines: the upper neck.
The core idea
Rest helps the brain heal. But if part of the injury is in the neck — and the neck is never examined or treated, then no amount of brain rest will resolve the part of the problem that was never about the brain. For many stalled PCS cases, that unaddressed upper-neck injury is the missing piece.
One impact, two injuries
To understand why the neck is so often involved, picture how a concussion actually happens. A concussion is caused by a force to the head, a blow, or a rapid acceleration and deceleration, like the head snapping during a car accident, a fall, or a sports collision. The brain moves inside the skull, and that's the brain injury.
But the head doesn't float in space. It sits on top of the neck, specifically on the delicate, highly mobile upper cervical spine. Any force strong enough to move the brain inside the skull also whips the neck. The same physics that injures the brain transmits straight into the joints, ligaments, and muscles of the neck, the identical mechanism that causes whiplash. You cannot concuss the brain without also loading the neck. The injury to the head and the injury to the neck happen in the same instant, from the same force.
This isn't a fringe idea. The medical literature describes it plainly: any significant blunt impact or acceleration/deceleration of the head produces inertial loading of the neck, which can result in sprain–strain injury to the soft tissues and joints of the cervical spine occurring concurrently with the head trauma. In other words, "concussion" and "neck injury" are frequently two names for two halves of a single event.
And the part of the neck most exposed to this force is the very top — the craniocervical junction, where the skull meets the first two vertebrae (the atlas and axis). This region carries the full weight and leverage of the head, which makes it the area that absorbs the most strain when the head is thrown. It's also the most neurologically critical region of the entire spine, which is why an injury there has outsized consequences.
Why the neck injury gets missed
If the neck is injured at the same time as the brain, why doesn't everyone get their neck examined? A few reasons:
The brain injury dominates the conversation. When someone has hit their head, all attention appropriately, goes to ruling out a serious brain bleed. The neck, especially the subtle upper-neck joint injury, gets overshadowed.
Standard imaging often looks normal. CT and MRI are excellent at detecting fractures and bleeds, but a functional misalignment or joint dysfunction at the top of the neck frequently doesn't show up on a routine scan. "Your scans are clear" can be true and yet miss the structural problem entirely.
The symptoms are blamed on the brain. Because neck-driven symptoms and brain-driven symptoms look nearly identical (more on that below), the headaches, dizziness, and fog get attributed to the concussion, and the neck is never considered.
Concussion care and neck care are different specialties. The cornerstone of concussion management is rest and graded return to activity. The neck, which often needs hands-on evaluation and care, falls outside that protocol.
The result: a person can do everything right by concussion guidelines and still not improve, because the neck component of their injury was never on anyone's radar.
How an upper-neck injury interferes with the nervous system
The upper neck isn't just a stack of bones — it's one of the most neurologically dense and sensitive regions in the body, and its proper alignment matters for the central nervous system in ways most people never realize. When the top of the neck is misaligned or its joints are irritated after a head-and-neck injury, it can interfere with the nervous system through several overlapping routes:
Distorted position-sense signals - Proprioception
The joints and muscles of the upper neck are densely packed with sensors that constantly tell the brain where the head is in space, called proprioception. The brain relies on this stream of information to coordinate balance, eye movement, and posture. When an injury distorts these signals, the brain receives faulty information, and the mismatch between what the neck reports, what the eyes see, and what the inner ear senses produces dizziness, imbalance, visual difficulty, and a foggy, disoriented feeling. Many "concussion" symptoms are, at their root, this sensory mismatch.
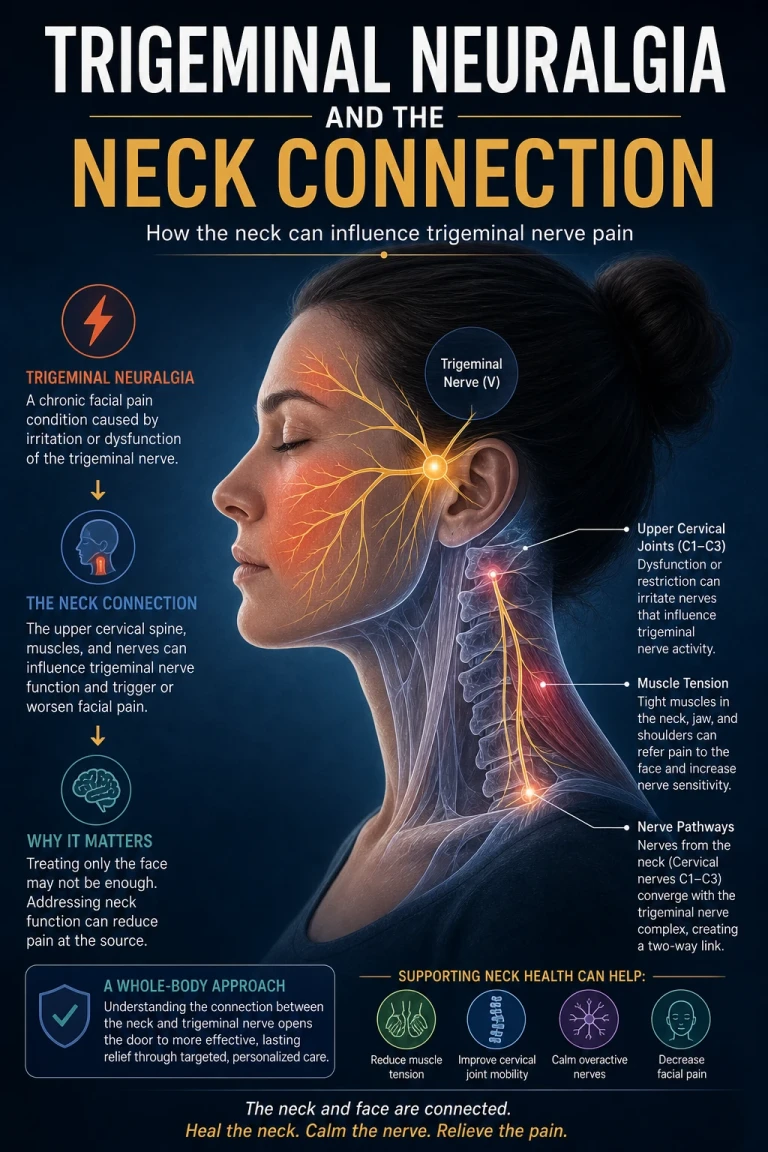
Shared nerve pathways with the head and face
The nerves of the upper neck feed into the same brainstem junction (the trigeminocervical complex) as the nerves of the head and face. Irritation from an injured upper neck can therefore be felt as headaches, facial pain, and pressure, symptoms easily mistaken for purely brain-based ones.
Strain on the brainstem and circulatory neighborhood
The craniocervical junction is the corridor through which the brainstem transitions into the spinal cord, and through which key blood vessels travel to and from the brain. The brainstem governs many of the automatic functions,heart rate, blood pressure, sleep, alertness, that are so often disrupted in PCS. Persistent irritation and altered mechanics at this junction can place ongoing stress on this critical region, which may help explain why so many PCS symptoms are autonomic (fatigue, poor sleep, light and noise sensitivity, difficulty regulating) rather than purely cognitive.
In plain terms
The top of the neck is where the body's wiring is most concentrated and most exposed. A misalignment there doesn't just cause neck pain, it can feed distorted signals into the balance system, the headache pathways, and the brainstem centers that run your body on autopilot. That's a lot of "brain" symptoms coming from a structural neck problem.
The full symptom picture of post-concussion syndrome
PCS is notorious for its long and varied symptom list, which is part of why it's so often misunderstood. Symptoms generally fall into four overlapping categories. Many people experience symptoms across all four at once.
Physical / somatic
Headaches (often daily or near-constant)
Neck pain or stiffness
Dizziness or lightheadedness
Balance problems and unsteadiness
Nausea
Fatigue and low energy
Sensitivity to light
Sensitivity to noise
Ringing in the ears (tinnitus)
Blurred or strained vision
Pressure or fullness in the head
Reduced exercise tolerance
Cognitive
Brain fog / mental cloudiness
Difficulty concentrating
Memory problems
Slowed thinking or processing
Trouble finding words
Mental fatigue with tasks
Feeling easily overwhelmed
Difficulty multitasking
Emotional / mood
Irritability
Anxiety or nervousness
Low mood or depression
Emotional volatility
Restlessness
Feeling "not like myself"
Sleep / autonomic
Trouble falling or staying asleep
Sleeping more than usual
Unrefreshing sleep
Heart-rate or blood-pressure changes with position
Temperature regulation issues
Feeling "wired and tired"
Look closely at that list and notice something striking: nearly every one of these symptoms, headaches, dizziness, balance trouble, visual disturbance, nausea, fatigue, ringing ears, cognitive fog — is also a documented symptom of upper cervical injury and whiplash. That overlap is the entire point of this article.
Why the symptom overlap matters so much
The medical literature is direct about this: there is considerable overlap among the signs and symptoms of mild traumatic brain injury, post-concussion syndrome, and whiplash injury to the neck. Injury or dysfunction of the cervical spine has been shown to cause headaches, dizziness, loss of balance, nausea, visual and auditory disturbances, and reduced cognitive function — the very symptoms typically considered synonymous with concussion.
This creates a genuine diagnostic trap. When a person who hit their head has headaches and brain fog, the natural assumption is "it's the concussion." But those identical symptoms can be produced by the neck injury that happened in the same instant. Without examining the neck, there's no way to know how much of the problem is brain and how much is cervical — and the two are managed completely differently. Brain injury calls for rest and graded recovery; cervical dysfunction calls for hands-on evaluation and care. Treat a neck problem with brain rest alone, and it simply doesn't resolve.
"85–90%of concussions resolve with standard rest-based care"
"85%of patients with PCS lasting beyond 10 days showed moderate-to-severe pain on manual testing of the upper cervical spine in published findings"
One event the same impact injures both brain and neck simultaneously. That last figure is the one that should change the conversation. If the great majority of people whose concussion symptoms persist also have a painful, dysfunctional upper neck on examination, then the upper neck isn't an occasional footnote in PCS, it's a leading suspect in exactly the cases that don't get better. The honest framing isn't that every PCS case is "really" a neck problem; it's that the neck is the component that routinely goes unexamined, and that's why the stubborn cases stay stubborn.
Why clearing the upper neck matters for recovery
Here's the recovery logic, and it's straightforward. The body has a remarkable capacity to heal — including the brain. But healing requires the right conditions. If the upper neck is misaligned and continuously feeding distorted, irritated signals into the central nervous system, it acts like persistent static on the line: the nervous system is being asked to recover while a constant source of interference keeps it stirred up.

Addressing that interference removes an obstacle to recovery. When the upper neck's alignment and movement are restored, the distorted position-sense signals can normalize, the headache pathways can quiet, and the strain on the brainstem corridor can ease — giving the nervous system a calmer environment in which to do its own healing. For someone whose recovery has stalled, this can be the difference between staying stuck and finally moving forward.
This is why, in persistent post-concussion cases, getting the upper neck evaluated and, where appropriate — corrected can be such an important step. It doesn't replace the brain's need to heal; it removes a structural roadblock that may have been quietly preventing that healing all along. The goal is to give the body the clearest possible path to recover the way it's designed to.
The recovery principle
You can't fully heal while a source of nervous-system interference goes unaddressed. Clearing the upper neck doesn't force recovery, it removes an obstacle to it, so the body's own healing can finally take hold.
Where upper cervical care fits
Upper cervical chiropractic focuses specifically on the alignment and movement of the atlas and axis, the exact region most strained in a head-and-neck injury and most consequential for the nervous system. For someone with persistent post-concussion symptoms, the approach is built around finding and addressing the cervical component that standard concussion care leaves out.
In practice, that means a thorough evaluation followed, where appropriate, by gentle, precise corrections, not the forceful, high-velocity twisting many people associate with general chiropractic, which is particularly important in someone recovering from a head-and-neck injury. The aim is to restore balanced alignment at the top of the neck and reduce the irritation feeding into the nervous system, so the body has a clearer path to recover.
What upper cervical care does — and does not — do
Being precise about scope is essential, especially with an injury this significant:
Upper cervical care focuses on the cervical (neck) component of post-concussion symptoms — the part standard concussion care typically doesn't address.
It does not treat the brain injury itself or claim to repair brain tissue, and it does not cure post-concussion syndrome.
It is not a replacement for appropriate medical evaluation and concussion management. It works best as part of a coordinated approach.
It is not for the acute emergency phase — a recent head injury must first be medically evaluated to rule out serious brain injury before any neck care is considered.
For the right person — particularly someone with persistent symptoms whose neck has never been examined — addressing the upper neck can be a meaningful part of recovery. Individual results vary, and a thorough examination is the only way to know whether your upper neck is involved in your case.
Our approach in Sarasota
At Sarasota Upper Cervical, post-concussion care begins with evaluation, not treatment. We take a detailed history of the injury and your symptoms, and we examine how the top of your neck is aligning and moving, the assessment that so often gets skipped. If we find an upper cervical pattern that fits your persistent symptoms, we'll explain it in plain language and discuss whether gentle upper cervical care is appropriate for you.
We also believe in coordinated care. Post-concussion recovery often involves more than one provider, and we're glad to be one part of that picture — working alongside your physician and other members of your care team, and referring out when something falls outside our focus. The goal is simply to make sure the upper-neck piece of your recovery isn't the piece everyone forgot to check.
Has your post-concussion recovery stalled?
If you're still struggling months or years after a concussion and no one has examined your upper neck, an upper cervical evaluation can help identify whether the missing piece is in your neck.
Frequently asked questions
1.Can a neck injury cause post-concussion symptoms?

Yes. The same impact that concusses the brain also loads and can injure the neck, and injury or dysfunction of the cervical spine is documented to cause headaches, dizziness, balance loss, nausea, visual and auditory disturbances, and reduced cognitive function — the same symptoms attributed to concussion. When these symptoms persist, an unaddressed upper-neck injury is one important possible reason.
2.Why didn't my concussion get better with rest?
Rest resolves the large majority of concussions, but it addresses the brain, not the neck. If part of your injury is a misalignment or dysfunction at the top of the neck — which the same impact commonly causes — rest alone won't resolve that component. This is one reason a subset of people don't recover on the expected timeline, and why having the upper neck examined can be valuable.
3.My MRI and CT were normal. Could my neck still be the problem?
Possibly. CT and MRI are excellent for detecting fractures and bleeds, but a functional misalignment or joint dysfunction at the upper neck often does not appear on routine imaging. A normal scan rules out certain serious problems but does not rule out the kind of upper cervical dysfunction that can drive persistent symptoms, which is identified through hands-on examination.
4.Is upper cervical care safe after a concussion?
A recent head injury must first be medically evaluated to rule out serious brain injury before any neck care is considered. For persistent post-concussion symptoms after that acute phase, upper cervical care uses gentle, precise, low-force corrections rather than forceful twisting. Whether it's appropriate for you depends on a thorough individual evaluation.
5.Does upper cervical care cure post-concussion syndrome?
No. It does not cure post-concussion syndrome and does not treat the brain injury itself. It focuses on the cervical component of persistent symptoms — addressing irritation and alignment at the top of the neck to remove a source of nervous-system interference, so the body has a clearer path to recover. Results vary from person to person, and it works best as part of coordinated care.
6.Where can I get help for post-concussion symptoms in Sarasota?
Sarasota Upper Cervical serves the Sarasota and Bradenton area and focuses on the upper cervical contribution to persistent post-concussion symptoms. You can request a consultation to find out whether your upper neck is part of why your recovery has stalled, and we coordinate with your physician and care team when that's the right path.
References
Marshall CM, et al. The role of the cervical spine in post-concussion syndrome. The Physician and Sportsmedicine, 2015.
Leslie O, Craton N. Concussion: purely a brain injury? Clinical Journal of Sport Medicine.
Kennedy E, et al. Clinical characteristics and outcomes of treatment of the cervical spine in patients with persistent post-concussion symptoms: a retrospective analysis. Musculoskeletal Science and Practice.
Cheever K, et al. Cervical spine sensorimotor deficits persist in people post-concussion. NCBI / PMC.
Treleaven J. Sensorimotor disturbances in neck disorders affecting postural stability, head and eye movement control.
Bartsch T, Goadsby PJ. Anatomy and physiology of pain referral in the trigeminocervical complex.
This article is for general educational purposes only and does not constitute medical advice, diagnosis, or treatment, and it does not establish a doctor–patient relationship. Concussion and post-concussion syndrome require professional medical evaluation; a recent head injury must be medically evaluated to rule out serious brain injury. Results of upper cervical care vary from person to person, and no specific outcome is promised or guaranteed. Upper cervical care is intended to work alongside, not replace, appropriate medical care. If you have a recent head injury or worsening neurological symptoms, seek medical care promptly. Always consult your physician or other qualified health provider with questions about a medical condition.



Leave a comment