

Your Neck Pain Doctor — Finding and Correcting the Source
Neck pain is one of the most common reasons people seek care in Sarasota — and one of the most commonly misunderstood. For many people, neck pain is treated as a local muscle problem: rub it, stretch it, take something for it, and wait for it to settle. Sometimes that works. But when neck pain keeps coming back, spreads into headaches, or simply never fully resolves, it is usually a sign that the source of the problem has not been addressed.
Schedule Your Appointment
Schedule appointmentThis guide takes a deeper look at why the neck hurts — the joints, the curve, the discs, the muscles, and the critical junction at the top of the spine — and how upper cervical chiropractic focuses on correcting the underlying structural problems that so often drive chronic neck pain. Along the way we will look at specific conditions like torticollis, occipital neuralgia, and occipital headaches, and at everyday contributors like workplace ergonomics.
Ready to find the source of your neck pain? Schedule a free consultation to find out whether you are a candidate for upper cervical care. Call 941-259-1891 to get started.
Listen to one of out patient's recovery from chronic neck pain and other health problems by clicking here.
Why Neck Pain Is So Often a Structural Problem
The neck, the cervical spine, is a remarkable piece of engineering. Seven vertebrae support the full weight of your head (about 10 to 12 pounds), allow an enormous range of motion, and protect the spinal cord and the nerves and blood vessels traveling between your body and your brain. That combination of mobility, load-bearing, and the protection of vital neurological structures makes the neck both incredibly capable and genuinely vulnerable.
When neck pain becomes chronic, the issue is rarely just an irritated muscle. More often, several structural factors are interacting: the alignment and curve of the spine, the health of the joints and discs, the balance of the muscles, and the motion available at each level. A muscle that stays tight for months is usually responding to something, compensating for a joint that is not moving well, a curve that has flattened, or an alignment problem at the top of the neck. Treating only the muscle leaves that driver in place.
This is why upper cervical chiropractic focuses on the structure of the neck, and especially on its foundation, the top two vertebrae, the atlas (C1) and axis (C2). When that foundation is misaligned, the effects cascade downward through the entire cervical spine. Let us walk through the specific mechanisms, then tie them back together.
Joint Capsule Injury and Joint Instability
Each vertebra in your neck connects to its neighbors through small paired joints called facet joints. Like other joints in the body, each is wrapped in a sleeve of connective tissue called a joint capsule, which is richly supplied with nerve endings and helps hold the joint together while sensing its position and movement.
When the neck is injured, in a car whiplash accident, a fall, a sports collision, or even a single sharp wrenching motion — these joint capsules can be stretched or torn. Because the capsule is so densely innervated, capsule injury is a significant and frequently overlooked source of neck pain. Damaged capsular tissue can remain a pain generator long after the original injury, and it can disrupt the position sense the joint normally provides, which the nervous system depends on to coordinate movement.
Capsule injury can also contribute to joint instability — a state in which the joint moves more, or less predictably, than it should. When the structures that normally restrain a joint are compromised, the surrounding muscles often tighten protectively, trying to create stability that the ligaments and capsule can no longer provide on their own. That protective guarding is itself a source of pain and stiffness, and it can become a self-perpetuating cycle: instability leads to muscle guarding, guarding leads to altered motion, and altered motion leads to further irritation.
Upper cervical care approaches this region carefully. The goal is not to force motion into an irritated or unstable area, but to restore more normal alignment so the joints can function within their proper range — reducing the irritation that drives protective muscle guarding. Where genuine instability is present, careful evaluation determines what is appropriate, and care is always coordinated with the broader clinical picture rather than applied indiscriminately.
Loss of the Cervical Curve (Cervical Lordosis)
Viewed from the side, a healthy neck has a gentle backward C-shaped curve called the cervical lordosis. This curve is not cosmetic — it is structural. It allows the cervical spine to absorb and distribute the load of the head efficiently, like a spring, so that forces are shared across the vertebrae, discs, and joints rather than concentrated in one place.
When this curve is reduced, flattened, or even reversed — a pattern sometimes called "military neck" — the mechanics of the entire neck change. The head's weight is no longer balanced over the spine; instead it shifts forward, and the muscles at the back of the neck must work harder, continuously, just to hold the head up. This is why people with a lost curve so often describe a deep, aching fatigue in the neck and upper shoulders by the end of the day.
Loss of the cervical curve frequently traces back to the top of the neck. The position of the head on the atlas sets the tone for the curve below it. When the upper cervical spine is misaligned, the rest of the neck compensates, and over time that compensation can show up as a flattened or reversed curve. Addressing the alignment at the top is therefore central to addressing the curve as a whole.
Disc Injury From Lost Curve and Muscle Asymmetry
Between each pair of vertebrae sits an intervertebral disc — a tough outer ring surrounding a gel-like center — that acts as a cushion and spacer, allowing movement while absorbing load. Discs are healthiest when forces pass through them evenly. They tolerate balanced, well-distributed load very well; they tolerate concentrated, lopsided, or sustained abnormal load far less well.
This is where the lost curve and muscle imbalance become more than a comfort issue. When the cervical curve flattens, load that should be shared across the spring-like curve concentrates on the discs and the front of the vertebrae. At the same time, when the muscles on one side of the neck pull differently than the other — a muscular asymmetry — the discs are loaded unevenly, side to side. Over months and years, this kind of abnormal, asymmetric loading may contribute to accelerated disc wear, dehydration, and degeneration.
Related article
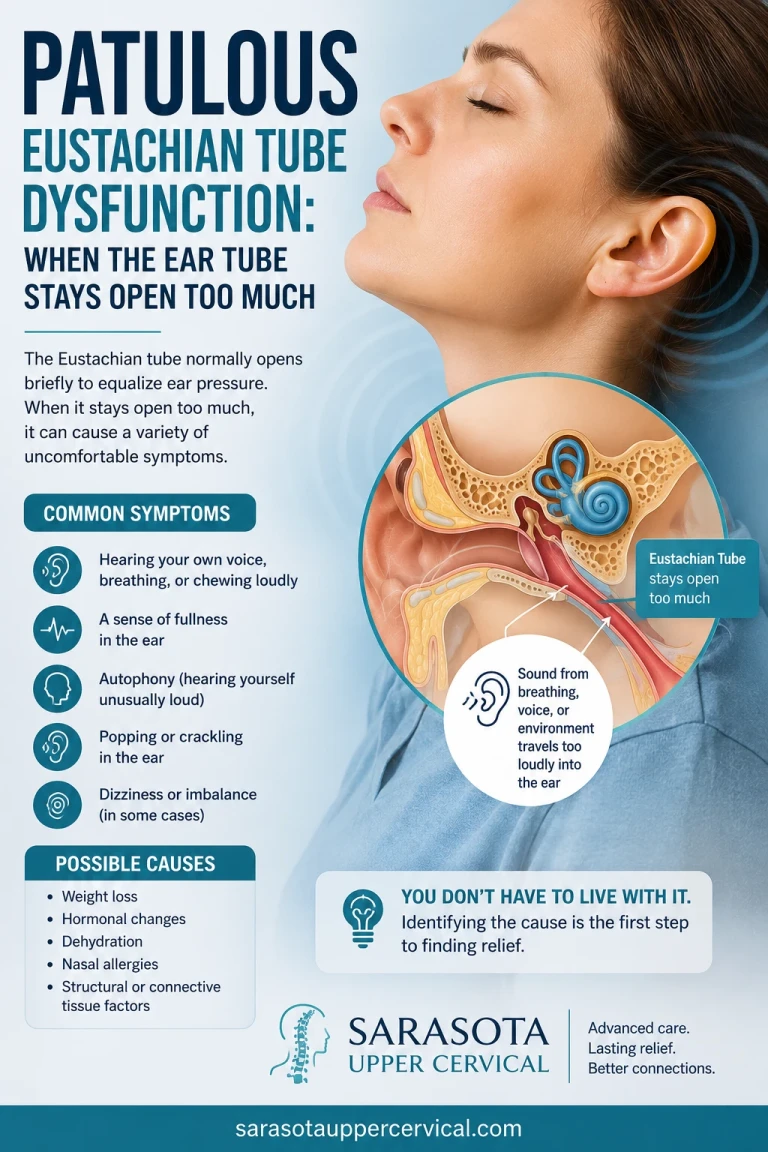
Patulous Eustachian Tube Dysfunction: When the Ear Tube Stays Open Too Much
May 26, 2026It is important to be precise here: this is a biomechanical contributing-factor relationship, not a claim that a single misalignment directly "causes" a herniated disc or that correction reverses existing disc damage. What the structural model says is reasonable and well-grounded: discs that are chronically loaded unevenly, because of a poor curve and unbalanced muscle pull, are working in conditions that favor faster wear. Restoring more normal alignment, a healthier curve, and more symmetric muscle function aims to give the discs a better mechanical environment going forward — which is a meaningful goal whether or not some wear has already occurred.
Occipital Muscle Tightness and Loss of Atlanto-Occipital Motion
Where the skull meets the spine sits the atlanto-occipital joint — the connection between the occiput (the base of the skull) and the atlas (C1). This joint is responsible for a large share of your head's nodding motion and for the constant fine adjustments that keep your eyes level and your head balanced. Tucked right around it are the small, deep suboccipital muscles that control and sense this delicate movement.
When the atlanto-occipital joint loses its normal motion — whether from injury, sustained poor posture, or upper cervical misalignment — these suboccipital muscles respond by tightening. Because they are small, deep, and densely packed with sensory receptors, sustained tightness here produces a very particular kind of discomfort: a tight, gripping tension at the very base of the skull, often with a sense of pressure or a headache that seems to radiate up the back of the head.
This region matters far beyond local tightness. The suboccipital muscles connect, through a structure called the myodural bridge, directly to the covering of the spinal cord — which is the subject of the next section. Restoring normal motion at the atlanto-occipital joint, by correcting the alignment that limits it, is a direct way to relieve the chronic tightness that builds up in this critical area.
The Myodural Bridge: A Direct Link From Muscle to Spinal Cord
One of the most important discoveries in modern neck anatomy is the myodural bridge, a dense band of connective tissue that physically connects the deep suboccipital muscles to the dura mater, the tough membrane that surrounds and protects the spinal cord and brain. In other words, there is a direct mechanical link between the small muscles at the base of your skull and the covering of your central nervous system.
Research has shown that this bridge is made largely of strong collagen fibers and that it serves real functions: it helps anchor and stabilize the dura as the head moves, and it appears to play a role in pumping cerebrospinal fluid — the fluid that bathes and nourishes the brain and spinal cord — as the suboccipital muscles contract during normal movement. The fact that this structure exists across many animal species suggests it serves a genuine, necessary purpose.
The clinical relevance for neck pain is direct. When the suboccipital muscles are chronically tight — for example, because the atlanto-occipital joint has lost its normal motion — that abnormal tension can be transmitted through the myodural bridge to the dura itself. This helps explain why tightness deep in the upper neck does not stay local: it can produce headaches, a sense of pressure in the head, and discomfort that is hard to pin to any single muscle. By focusing on the alignment and motion of the upper cervical spine, care aims to reduce the abnormal suboccipital tension that loads this bridge.
Ergonomics: How Your Workday Shapes Your Neck
Few things load the modern neck like the way we work. Hours spent looking down at a screen, a laptop set below eye level, a phone cradled against one shoulder, or a monitor positioned off to one side all ask the neck to hold non-neutral positions for long stretches. The further the head drifts forward and down from its balanced position over the spine, the more the muscles of the neck and upper back must work to support it.
This sustained postural load ties directly into the mechanisms already discussed. Prolonged forward-head posture works against the cervical curve, contributes to the flattening that concentrates load on the discs, and keeps the suboccipital muscles in a state of low-grade, continuous tension. An off-center setup that makes you rotate or side-bend to see your screen feeds the muscular asymmetry that loads the discs unevenly. In this sense, poor ergonomics is not a separate problem — it is a daily, repeated dose of exactly the forces that drive structural neck pain.
Practical ergonomic adjustments
• Raise your screen so the top of the monitor is at or slightly below eye level, keeping your head balanced rather than tilted down.
• Position your primary screen directly in front of you, not off to one side, to avoid sustained rotation.
• Bring your phone up to eye level for reading and texting instead of dropping your head to it, and use a headset rather than cradling it against your shoulder.
• Set your chair so your feet are flat, hips and knees roughly level, and forearms supported, which helps your whole spine stack more neutrally.
• Take regular movement breaks — even a few moments of looking up and gently moving the neck every half hour interrupts sustained loading.
Ergonomics alone will not correct an existing structural problem, but it removes a constant aggravating force — which makes it an essential partner to care rather than a substitute for it.
Specific Types of Neck Pain and Related Conditions
"Neck pain" is an umbrella term. Understanding which pattern you are dealing with helps clarify why an upper-cervical-focused approach can be relevant. Three conditions are worth describing specifically.
Torticollis
Torticollis — sometimes called wryneck — is a condition in which the neck twists or tilts to one side, often with significant muscle spasm, pain, and a markedly limited range of motion. It can come on suddenly, sometimes overnight, and the head may become locked in a rotated or side-bent position. Torticollis reflects a profound imbalance in the muscles that control head position, frequently linked to irritation and altered mechanics in the upper cervical spine. Because the atlas and axis govern so much of the neck's rotation, alignment problems in this region are closely tied to the muscular imbalance that drives torticollis. Care focuses on calming the irritation and restoring more normal alignment so the muscles are no longer locked in their protective, asymmetric pattern.
Related article
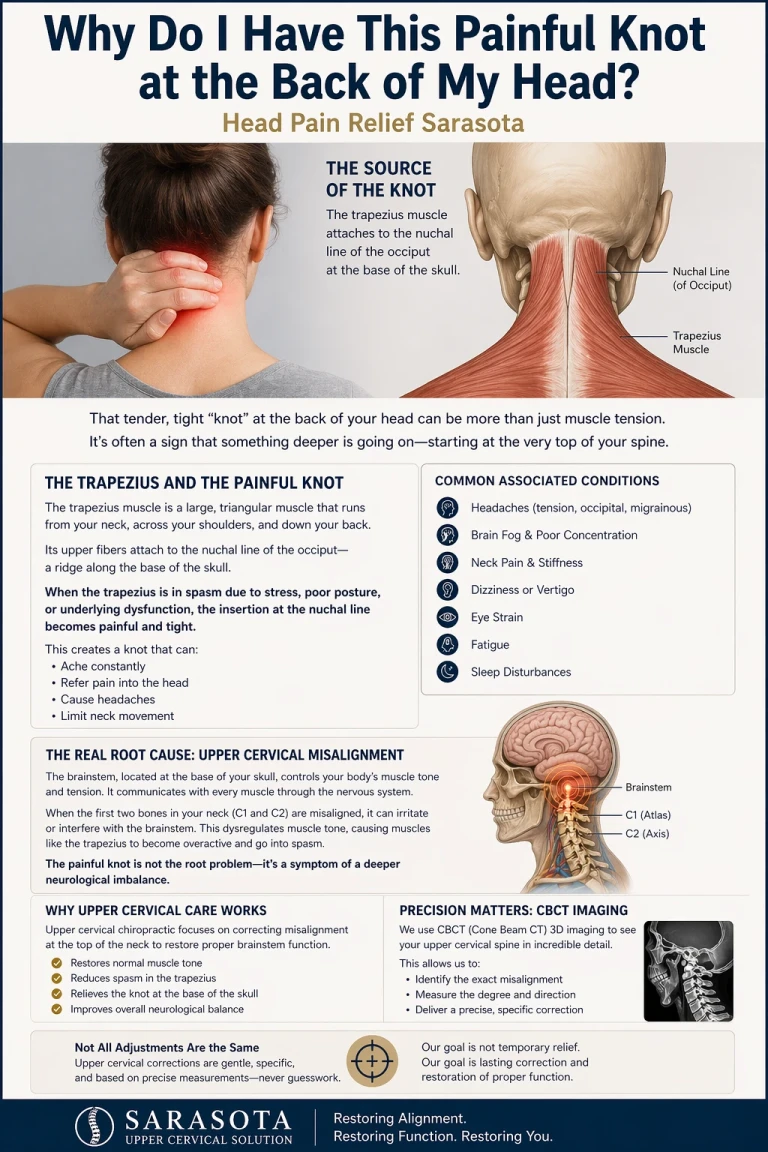
Why do I have this painful knot at the back of my head | Head Pain relief sarasota
Apr 23, 2026Neck pain and cervicogenic vertigo
Vertigo is commonly associated with neck pain. When the joints in the neck are injured, not only does it cause ibalances in muscle tone but it also causes abberrant input form the joint surface into the vestibular nucleus. The vestibular nucleus is the part of the nervous system that controls and coordinates sensory input form the ears, the eyes, and the neck modulating balances.
Occipital Neuralgia
Occipital neuralgia is a distinct kind of pain caused by irritation of the occipital nerves, which travel from the upper cervical spine up through the suboccipital muscles to supply sensation to the back and top of the head. The pain is often described as sharp, shooting, electric, or stabbing, starting at the base of the skull and shooting upward, sometimes accompanied by tenderness, tingling, or sensitivity of the scalp. Because these nerves pass directly through the upper cervical region and its muscles, misalignment and the resulting muscle tightness in this area can irritate them. An upper cervical approach focuses on reducing that mechanical irritation at its source rather than only numbing the downstream pain.
Occipital and Cervicogenic Headaches
Many headaches actually originate in the neck. Occipital headaches typically begin at the base of the skull and radiate up the back of the head, and they are closely related to the suboccipital tightness and occipital nerve irritation just described. More broadly, cervicogenic headaches are headaches whose source is the cervical spine — referred pain from the upper neck's joints, muscles, and nerves that is felt in the head. The shared thread is that the upper neck, when misaligned and mechanically irritated, can be the true generator of pain that is experienced as a headache. This is why addressing the structure of the upper cervical spine is so relevant for people whose headaches have a clear neck component.
Tying It Together: Correcting Upper Cervical Misalignment
Step back and a pattern emerges. Joint capsule injury and instability, a lost cervical curve, uneven disc loading from poor curve and muscle asymmetry, suboccipital tightness from restricted atlanto-occipital motion, tension transmitted through the myodural bridge, and conditions like torticollis, occipital neuralgia, and occipital headaches — these are not unrelated problems. They are connected, and they share a common foundation at the top of the neck.
The atlas and axis are the structural keystone of the cervical spine. They carry the head, set the tone for the curve below, govern much of the neck's rotation and nodding, and sit at the crossroads of the suboccipital muscles, the occipital nerves, and the myodural bridge. When this region is misaligned, the consequences ripple outward — which is precisely why upper cervical chiropractic focuses specifically on correcting misalignment of the atlas and axis.
By restoring more normal alignment at this keystone, care aims to: reduce the irritation that drives protective muscle guarding; allow a healthier head position and curve to be restored; promote more balanced, symmetric muscle function so loads are shared more evenly; restore normal motion at the atlanto-occipital joint and relieve suboccipital tightness; and reduce the abnormal tension carried through the myodural bridge. Rather than chasing each symptom separately, the approach addresses the shared structural source they stem from.
Precision Matters: 3D Imaging
Before any correction is made, detailed 3D imaging (CBCT scans) is used as a precision tool to analyze your individual anatomy and measure the exact position of the atlas. Because this region is small, deep, and structurally critical, this individualized, data-driven approach is essential. It allows the correction to be tailored precisely to your spine rather than applied generically.
Gentle Corrections — No Twisting, Popping, or Pulling
Upper cervical corrections are gentle and specific, performed with no twisting, popping, or cracking. This matters especially in a region this delicate, and for people whose joints are already irritated or guarding. The aim is to make a precise correction and allow the body to hold it over time, so the upper neck can stabilize and the structures below can recover a healthier pattern — not to deliver repeated forceful manipulation.
Candidacy Comes First
Not all neck pain comes from the upper cervical spine, and not everyone is a candidate for upper cervical care. A thorough evaluation is designed to determine whether your specific case shows the structural signs that make this approach appropriate — and to tell you honestly if it does not. That candidacy-first standard protects you and keeps the focus on what will actually help.
Who Should Consider an Evaluation?
An upper cervical evaluation may be worth considering if you experience any of the following:
• Neck pain that keeps returning or has never fully resolved despite other treatments
• Neck pain that began or worsened after a car accident, fall, sports injury, or whiplash
• Chronic tightness or pressure at the base of the skull
• Headaches that start in the neck or back of the head
• Sharp, shooting pain from the base of the skull up over the head (possible occipital neuralgia)
• A neck that twists or locks to one side (torticollis)
• A job or daily routine that keeps your head down or turned for long periods
Related article
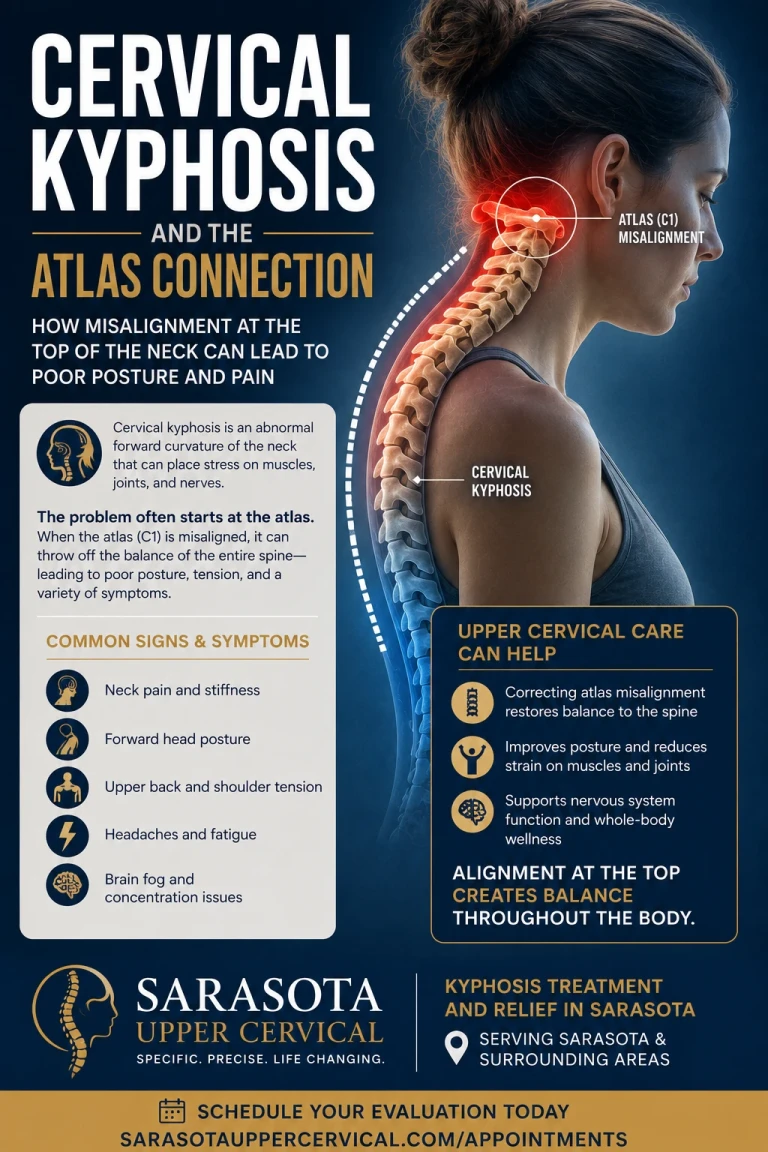
Cervical kyphosis and the atlas connection | Kyphosis treatment and relief sarasota
Jun 28, 2026Ready to find the source of your neck pain? Schedule a free consultation to find out whether you are a candidate for upper cervical care. Call 941-259-1891 to get started.
Frequently Asked Questions
Is upper cervical chiropractic safe for neck pain?
Upper cervical care uses gentle, specific corrections with no twisting, popping, or cracking, and begins with a thorough evaluation — including 3D imaging — to determine whether you are a candidate. This careful, individualized approach is designed with the delicacy of the upper neck in mind. As with any care, appropriateness is assessed case by case.
How is this different from regular chiropractic adjustments?
The main differences are focus and method. Upper cervical care concentrates specifically on the alignment of the top two vertebrae, the atlas and axis, which serve as the foundation for the rest of the neck. Corrections are gentle and precise rather than involving the forceful twisting or popping some people associate with general chiropractic, and they are guided by detailed imaging of your individual anatomy.
Can correcting my neck alignment really help my headaches?
Many headaches have a clear neck component. Occipital and cervicogenic headaches originate from the joints, muscles, and nerves of the upper neck, referring pain into the head. When misalignment in the upper cervical spine is irritating these structures, addressing that alignment focuses on a potential true source of the headache rather than only the symptom. A thorough evaluation determines whether your headaches have this kind of neck involvement.
What is the myodural bridge, and why does it matter for neck pain?
The myodural bridge is a dense connective-tissue link between the deep muscles at the base of the skull and the covering of the spinal cord. When these suboccipital muscles are chronically tight — often because the joint between the skull and the atlas has lost normal motion — that tension can be transmitted through the bridge. This helps explain why deep upper-neck tightness can produce headaches and a sense of head pressure, not just local soreness.
Will improving my workstation fix my neck pain on its own?
Good ergonomics is important because it removes a constant aggravating load on the neck, but it generally will not correct an existing structural problem by itself. Think of it as an essential partner to care: ergonomics reduces the daily forces working against you, while care addresses the underlying alignment and mechanics. Together they give your neck the best chance to recover and stay better.
Can upper cervical care reverse disc degeneration or a flattened curve?
It is most accurate to think of the goal as improving the mechanical environment of the neck rather than promising to reverse existing wear. By working toward more normal alignment, a healthier curve, and more balanced muscle function, care aims to reduce the abnormal, uneven loading that contributes to disc wear and to support a better curve going forward. What is appropriate and realistic in your case is determined by evaluation, including imaging.
How do I know if I'm a candidate?
The best first step is a consultation and evaluation. This assessment, which may include 3D imaging to measure the position of your atlas, is designed to determine whether your neck pain has the structural signs that upper cervical care addresses. If it does not, you will be told so.
You can schedule a free consultation by calling 941-259-1891.
This content is for informational purposes only and does not constitute medical advice. Sarasota Upper Cervical focuses on correcting upper cervical misalignments; individual results vary, and candidacy for care is determined by evaluation.



Leave a comment