
If you’re living with POTS or another form of dysautonomia, you already know how much it can take over daily life, the racing heart when you stand, the lightheadedness, the fatigue that no amount of rest seems to fix, the brain fog, and the frustration of being told your test results look “normal.”
Many patients in Sarasota arrive at our office after years of specialist visits and treatment trials, still searching for answers. This guide is here to explain one piece of the picture that is often overlooked: the connection between the upper cervical spine — the top of your neck, where the skull meets the atlas (C1) and axis (C2) — and the autonomic nervous system that governs heart rate, blood pressure, and so much more. It’s an emerging, biologically grounded area of care, and understanding it may help you ask better questions about your own case.
Schedule Your Appointment
Schedule appointmentA notable anatomical finding over the past two decades, known as the myo-dural bridge, gives one mechanism for how connecctive tissue in the upper cervical region can cause mechanical tension on the brainstem leading to autonomic dysfunction.
A note before we begin, because it matters: upper cervical care is best understood as a complementary approach that focuses on a potential structural contributor to autonomic dysfunction. It is not a cure, and it is not a replacement for the care of your cardiologist, neurologist, or other physicians. Nothing here should be taken as a reason to stop prescribed treatment. The goal is to add a piece that may be missing, not to remove the ones that are working.
If you’re living with POTS or dysautonomia and want to explore whether the upper neck is part of your picture, schedule a free consultation — book here or call 941-259-1891 to see if you’re a candidate for care.
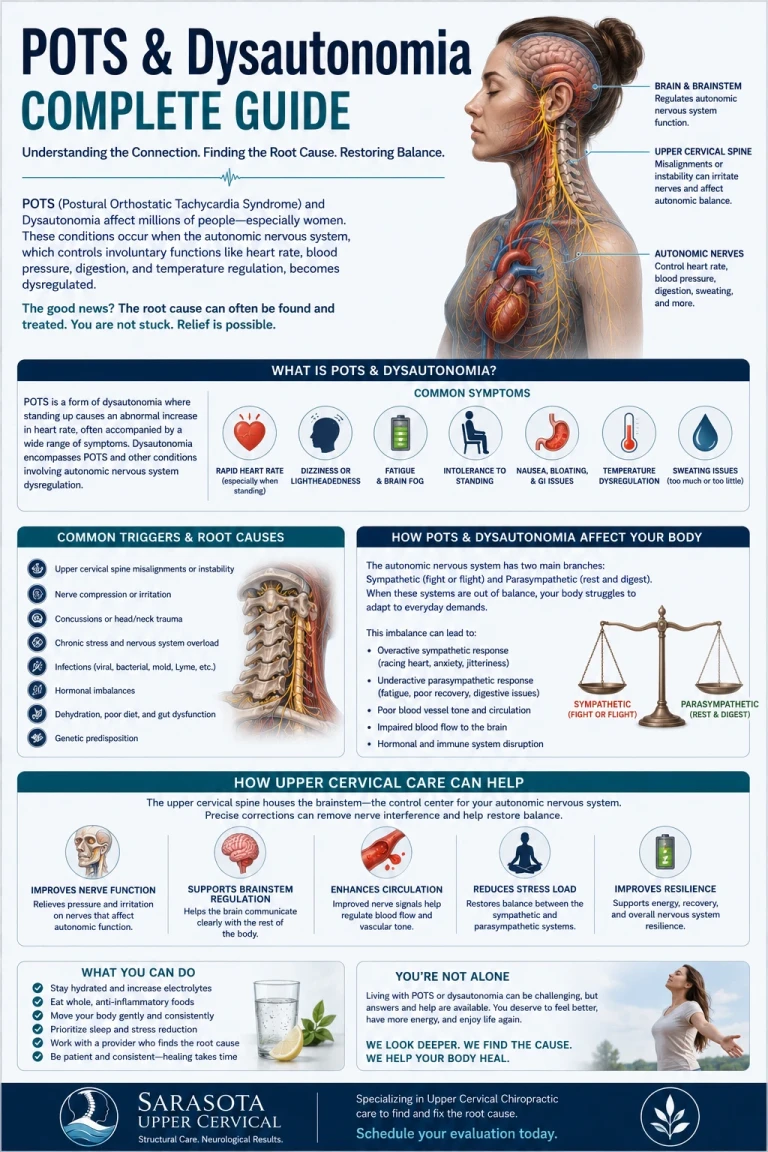
What Are POTS and Dysautonomia?
Dysautonomia is an umbrella term for dysfunction of the autonomic nervous system (ANS) — the part of your nervous system that runs automatically, in the background, without your conscious input. The ANS regulates heart rate, blood pressure, digestion, body temperature, breathing, and the constant adjustments your body makes to keep itself in balance. POTS, postural orthostatic tachycardia syndrome, is the most common and widely recognized form of dysautonomia. Its hallmark is an abnormal increase in heart rate when moving from lying or sitting to standing, often accompanied by lightheadedness, palpitations, fatigue, brain fog, and sometimes fainting. It tends to affect women disproportionately, frequently young and otherwise healthy, and it can be genuinely disabling. Because the autonomic nervous system touches nearly every organ, dysautonomia rarely shows up as a single symptom. Patients often describe a constellation: the cardiovascular symptoms most associated with POTS, plus digestive issues, temperature dysregulation, sleep disruption, exercise intolerance, and cognitive difficulties. That whole-body quality is exactly what you’d expect from a system whose job is whole-body regulation.
The Autonomic Nervous System and the Brainstem
To understand why the upper neck may matter, you have to look at where the body’s autonomic control sits. Much of the autonomic nervous system is coordinated by the brainstem, the structure at the base of the brain that connects to the spinal cord. The brainstem contains key autonomic control centers, including a region called the nucleus tractus solitarius that helps regulate heart rate and blood pressure. The brainstem is also the origin point for the majority of the cranial nerves, including the vagus nerve, the main highway of the parasympathetic (“rest and digest”) system. Here is the anatomical fact that makes the upper neck relevant: the brainstem does not sit in some remote, protected corner of the body. It passes directly through the junction between the skull and the upper cervical spine — the region governed by the atlas (C1) and axis (C2). These two vertebrae form a uniquely mobile, uniquely vulnerable passageway for the brainstem, spinal cord, blood vessels, and nerves that all converge there.
How the Upper Neck May Influence Autonomic Function
When the atlas and axis are misaligned or unstable, several mechanisms have been proposed for how that could ripple outward into autonomic symptoms. These are areas of active study, and we present them as proposed mechanisms rather than settled fact: Brainstem irritation. Misalignment at the craniocervical junction may create irritation near the brainstem regions that regulate heart rate, blood pressure, and vascular tone, potentially contributing to the instability that defines POTS. Vagus nerve involvement.
Related article
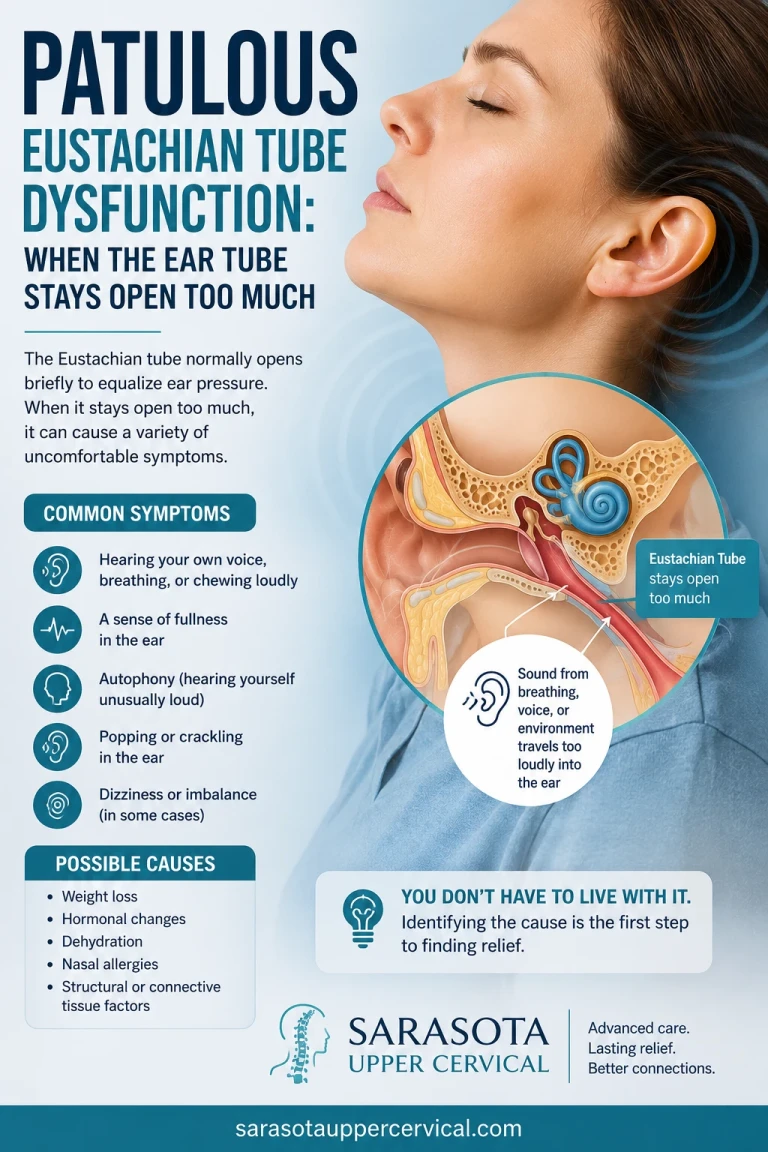
Patulous Eustachian Tube Dysfunction: When the Ear Tube Stays Open Too Much
May 26, 2026The vagus nerve exits the skull near the upper cervical region. Because it carries the bulk of parasympathetic signaling, irritation in this area has been proposed as a contributor to the imbalance between the "fight or flight" and "rest and digest" systems that many dysautonomia patients experience. Blood flow and fluid dynamics. The upper cervical region is a critical junction for blood flow to and from the brain and for cerebrospinal fluid movement. Altered alignment may affect these dynamics, which are closely tied to how the body manages pressure and posture. The common thread is that the upper neck is anatomically positioned to influence the very systems that go awry in dysautonomia. That positioning is why this connection is being taken seriously.
The Craniocervical Instability and EDS Connection
One of the most studied links between the neck and dysautonomia involves craniocervical instability (CCI) and Ehlers-Danlos syndrome (EDS), a group of connective tissue disorders that cause ligament laxity throughout the body. When the ligaments at the craniocervical junction are too loose, the result can be excessive movement at the top of the neck, and CCI is known to coexist with POTS at notably high rates.
In one neurosurgical study of EDS patients with instability at the C1-C2 level, every patient experienced lightheadedness and many had fainting that persisted despite maximal medical management; after surgical stabilization of that junction, autonomic symptoms improved significantly. It’s important to be precise about what that study does and does not show. It demonstrates that the structural integrity of the craniocervical junction can meaningfully affect autonomic functio, powerful evidence that this region matters. It does not show that chiropractic correction produces the same result as surgery; that was a surgical intervention in a specific, severe population.
What it offers is a strong reason to take the neck-autonomic relationship seriously, and to evaluate it carefully in the right patients. What the Evidence Does and Doesn’t Say We believe in being straight with patients about the state of the science, because you’ve likely been given more certainty than the evidence supports — in both directions. The biological plausibility for an upper cervical influence on autonomic function is strong, grounded in well-established anatomy: the brainstem’s autonomic centers, the cranial nerves, and the vascular and fluid pathways all converge at the top of the neck. There is supporting evidence from blood pressure studies, heart rate variability research, case reports, and the craniocervical instability literature.
At the same time, large-scale randomized controlled trials specifically testing upper cervical chiropractic for POTS and dysautonomia have not yet been published. The evidence is promising and growing, but it is not yet at the level of definitive proof. Anyone who tells you upper cervical care is a guaranteed cure for POTS is overstating what is known. Our position is the honest middle: a biologically reasonable, complementary approach worth evaluating — not a miracle, and not a replacement for your medical team.
Why Candidacy and Careful Evaluation Come First
Dysautonomia has many causes and contributors, and the upper neck is only one possible piece. Not everyone with POTS has a structural cervical component, and not everyone is a candidate for upper cervical care. That’s precisely why a responsible evaluation comes before any conclusions. Certain patterns make an upper cervical involvement more worth investigating, including: Symptoms that began or worsened after a head or neck injury, whiplash, or concussion A diagnosis of EDS, hypermobility, or connective tissue laxity.
Neck pain, headaches, or dizziness alongside the autonomic symptoms. Symptoms that have not responded well to standard management. A history of trauma to the upper neck region If your evaluation suggests the upper neck is not a meaningful contributor in your case, you deserve to know that, so you don’t invest time and hope in the wrong direction. Candidacy-first care protects you.
Precision Matters: 3D Imaging and Customized Corrections
One of the defining features of upper cervical care is its precision. Before any correction is considered, detailed 3D imaging (CBCT scans) is used as a precision tool to analyze your individual anatomy and measure the exact position of the atlas. For a complex, multi-system presentation like dysautonomia, that individualized, data-driven approach is essential — this is not a one-size-fits-all method.

No Twisting, Popping, or Pulling
Many people picture forceful adjustments when they think of chiropractic. Upper cervical care is different. Corrections are gentle and specific, performed with no twisting, popping, or cracking, and designed to allow the body to hold the correction over time. For a dysautonomia patient whose nervous system is already dysregulated and sensitive, this gentle, low-force approach is particularly important. The goal is not endless repeated visits — it is the right correction, held and stabilized, so the body has the chance to function more normally.
What to Expect, and a Realistic View of Progress
Because dysautonomia is a whole-body regulatory problem, change — when it happens — tends to be gradual rather than instant. Holding a correction over time is what allows the nervous system room to recalibrate. We track progress honestly: needing fewer corrections over time is a sign the body is stabilizing, not a reason to keep coming in. And throughout, upper cervical care works alongside your existing medical care.
Take the First Step Toward Answers
If you’ve been managing POTS or dysautonomia and the upper neck has never been part of the conversation, that’s a gap worth closing — especially if your symptoms followed a neck injury or you have a connective tissue diagnosis.
Schedule your free consultation today to find out whether you’re a candidate for upper cervical care as a complementary part of your overall plan. Book here or call 941-259-1891 to get started.
Learn More
This guide is the hub for our POTS and dysautonomia content. For related reading on how the upper neck connects to other symptoms many dysautonomia patients share, explore our articles on:
Dizziness and the upper cervical connection, brain fog and upper neck misalignment, and our complete guide to tinnitus and the neck connection.
Frequently Asked Questions
Related article
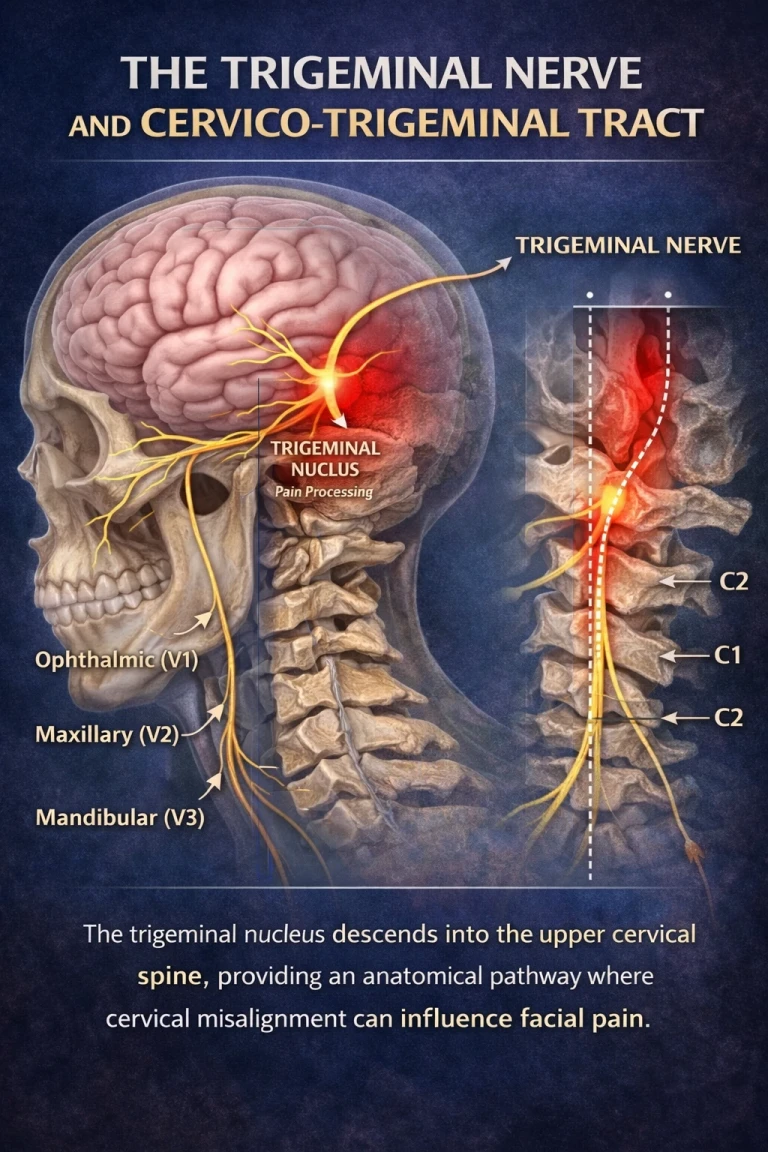
Trigeminal Neuralgia: The Anatomy of the “Suicide Disease” Sarasota Trigeminal Neuralgia Relief
Apr 10, 20261. Can upper cervical chiropractic cure POTS or dysautonomia?
No. Upper cervical care is a complementary approach that focuses on a potential structural contributor to autonomic dysfunction — it is not a cure and not a replacement for medical care. Large-scale clinical trials specifically for POTS have not yet been published, though the underlying anatomy provides strong biological plausibility and the evidence is growing.
2. How could a problem in my neck affect my heart rate and blood pressure?
The brainstem, which contains key autonomic control centers and is the origin of most cranial nerves including the vagus nerve, passes through the junction between the skull and the upper neck. Misalignment or instability of the atlas and axis may irritate this region, which is why the upper neck can be relevant to autonomic symptoms.
3. I have EDS. Is that relevant?
It may be. Connective tissue laxity from EDS can predispose people to craniocervical instability, which coexists with POTS at high rates. This makes a careful evaluation of the upper neck particularly worth considering, though candidacy is always assessed individually.
4. Will I need to stop my current POTS treatment?
We have many POTS cases that either recover or imporve markedly after undergoing upper cervical chiropractic care. You should not stop conventional treatment but upper cervcial care can be a supportive approach.
5. How do I know if I’m a candidate?
A thorough evaluation, which may include 3D imaging to assess the alignment of the atlas, is used to determine whether your upper neck is likely a meaningful contributor. Patterns such as symptom onset after a neck injury, a connective tissue diagnosis, or accompanying neck pain and dizziness make it more worth investigating.
Schedule a free consultation or call 941-259-1891 to find out. Book online here.
This content is for informational purposes only and does not constitute medical advice. It is not intended to diagnose, treat, or replace care provided by your physicians.



Leave a comment